Introduction
Tracheostomy care is an essential aspect of airway management for patients requiring long-term ventilation or respiratory support, yet it remains a complex and critical procedure. In many resource limited settings, the primary care workforce which includes general practitioners (GPs) are vital in supporting tracheostomy management, particularly in emergencies and given the scarcity of otolaryngology subspecialists.1 However, GPs in such settings often face substantial challenges in managing these procedures due to a number of factors including lack of formal training.1,2 Healthcare providers in low- and middle-income countries (LMICs) report low levels of comfort and confidence when performing critical airway management procedures, such as tracheostomy care.3–5 In a study conducted by Nyanzi et al. (2023), clinicians in Uganda reported inadequate training in tracheostomy management, leading to suboptimal care and increased risk for patients.6 Furthermore, healthcare providers in LMICs report limited access to specialized training more broadly, advanced equipment, and hands-on experience, leading to low confidence and competence in performing critical procedures such as tracheostomy management.7
Simulation-based training has emerged as a promising solution to address these gaps in clinical education. Low-cost, high-anatomical models are effective in improving healthcare workers’ skills, confidence, and patient care outcomes.8,9 3D-printed models have successfully simulated complex medical procedures such as cricothyrotomy, chest tube insertion, and temporal bone dissection, providing a safe, cost-effective alternative to traditional methods.10 The use of 3D-printed models in airway management training improved practitioners’ technical skills, alleviated discomfort, and enhanced clinical knowledge, providing an effective means of knowledge sharing between providers and patients through hands-on practice in a controlled, risk-free environment.11,12
This project seeks to develop a novel low-cost, high anatomical fidelity 3D-printed tracheostomy model to enhance simulation-based training for GPs in Rwanda. A competency-building tracheostomy training model holds promise for broader application across LMICs and low-resource healthcare environments as a tool to teach and reinforce essential management of tracheostomy care for all health care providers.
Methods
Study Design
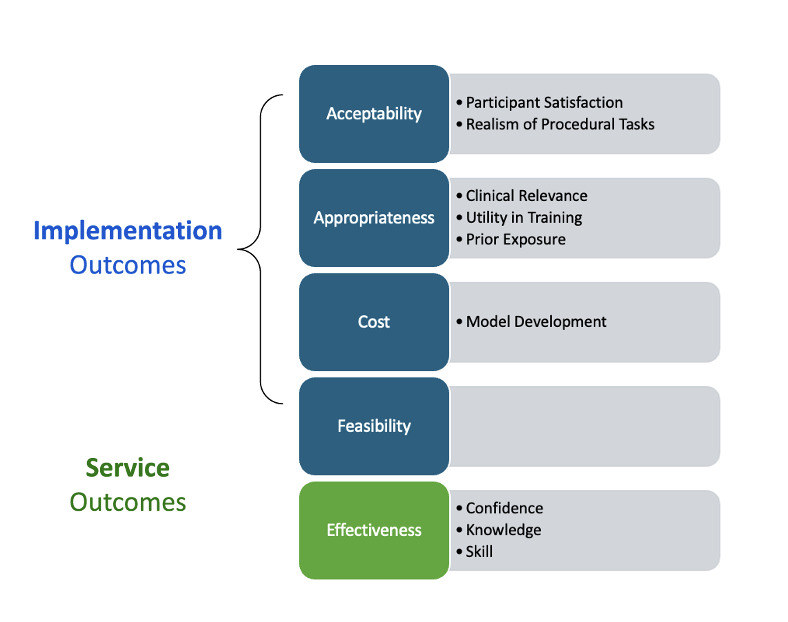
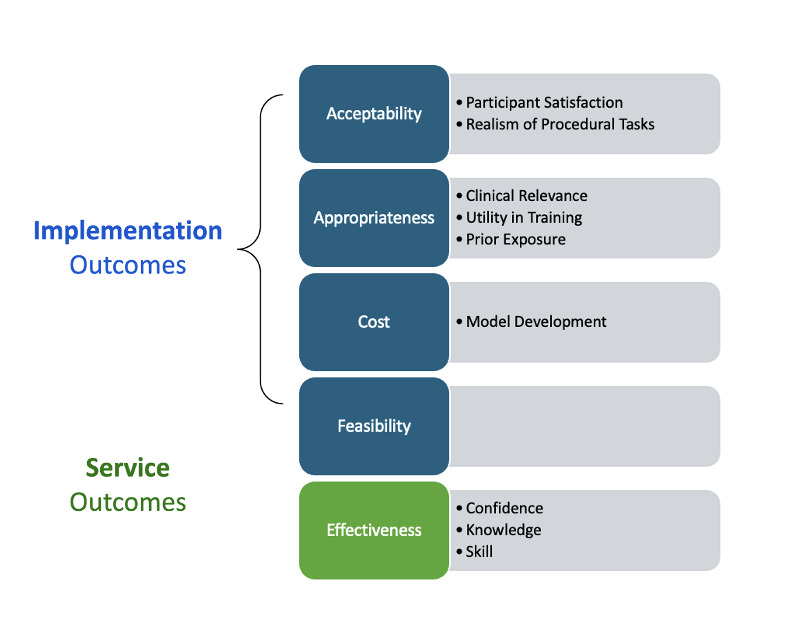
The development and evaluation of the 3D-printed tracheostomy model were conducted as a Type II effectiveness-implementation study, which simultaneously assessed the training’s impact and evaluated implementation outcomes such as acceptability, feasibility, adoption, and cost. Additionally, the service outcome of effectiveness was evaluated through knowledge, confidence, and skill. The study was carried out in two phases: an initial pilot phase with subspecialists and a subsequent simulation training event for GPs from across Rwanda (Figure 1).
The pilot phase aimed to assess the acceptability and relevance of the model among local otolaryngologists, while the training event focused on evaluating the effectiveness of the model in improving tracheostomy management skills in a real-world training environment. These evaluated domains are summarized in Figure 2.
Initial Review by ENT Providers
We first sought feedback from local ENT providers in Rwanda to ensure the model’s accuracy and relevance to clinical practice. Five ENT practitioners evaluated the model based on its fidelity to real-life clinical scenarios, including its anatomical accuracy, functionality (such as the ability to perform suctioning, decannulation, and tracheostomy replacement), and overall usability. The ENT providers completed a structured questionnaire that addressed 1) relevance to real-life scenarios, 2) anatomical accuracy, 3) usability, and 4) functionality. The feedback collected from the ENT providers served to refine the model to assess whether it met the needs of healthcare providers in Rwanda.
Simulation Training Event
Following the pilot phase, the model was tested in a simulation course for GPs on April 4-5, 2025, held at the University of Global Health Equity (UGHE) in Kigali, Rwanda. The event provided 40 GPs from around Rwanda with a hands-on opportunity to practice critical tracheostomy management skills using a 3D-printed model coupled with didactics and coaching from ENTs.
The simulation training focused on key aspects of tracheostomy care including accidental decannulation, suctioning, tracheostomy tube tie placement, and tracheostomy tube replacement. A pre- and post-training survey assessed changes in participants’ knowledge, skill, comfort, and confidence in tracheostomy care. The survey consisted of demographics, knowledge, self-perceived skill, comfort/confidence, utility of training, and prior exposure (Supplemental Material). Additionally, participant performances were video recorded before and after training and then rated with a rubric. This rubric was adapted to assess the skills taught at our training and to the Rwandan health setting from the Objective Structured Assessment of Technical Skills (OSATS), which is commonly used to assess surgical skills, as well as existing airway management simulation assessment tools.13–15
Data Analysis
Data from the pre/post surveys were analyzed quantitatively using paired t-tests or non-parametric equivalents to assess significant differences in participants’ knowledge, skill, and comfort levels before and after the intervention. Additionally, qualitative feedback from open-ended questions was analyzed thematically.
Ethical Considerations
The Rwandan Institutional Review Board at the Rwanda National Ethic Committee (RNEC) approved this study (study #: 00001497). All participants in the simulation training event provided written informed consent.
Results
Participant Demographics
Forty GPs from across Rwanda participated in the ENT simulation training course held at the University of Global Health Equity (UGHE) in Kigali on April 4-5, 2025. Participant demographic data is summarized in Table 1.
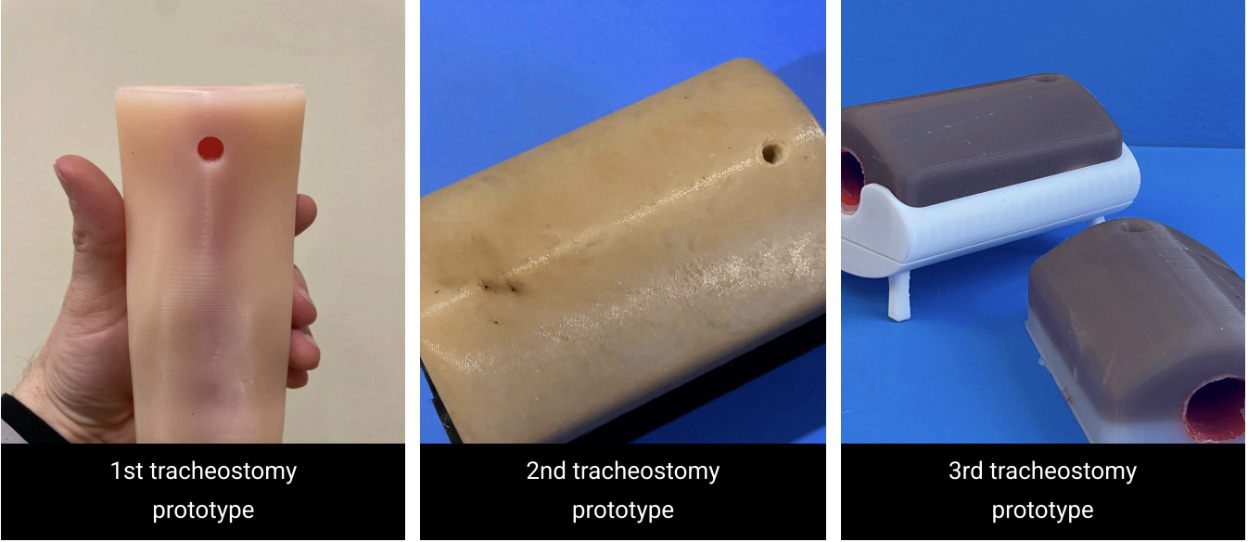
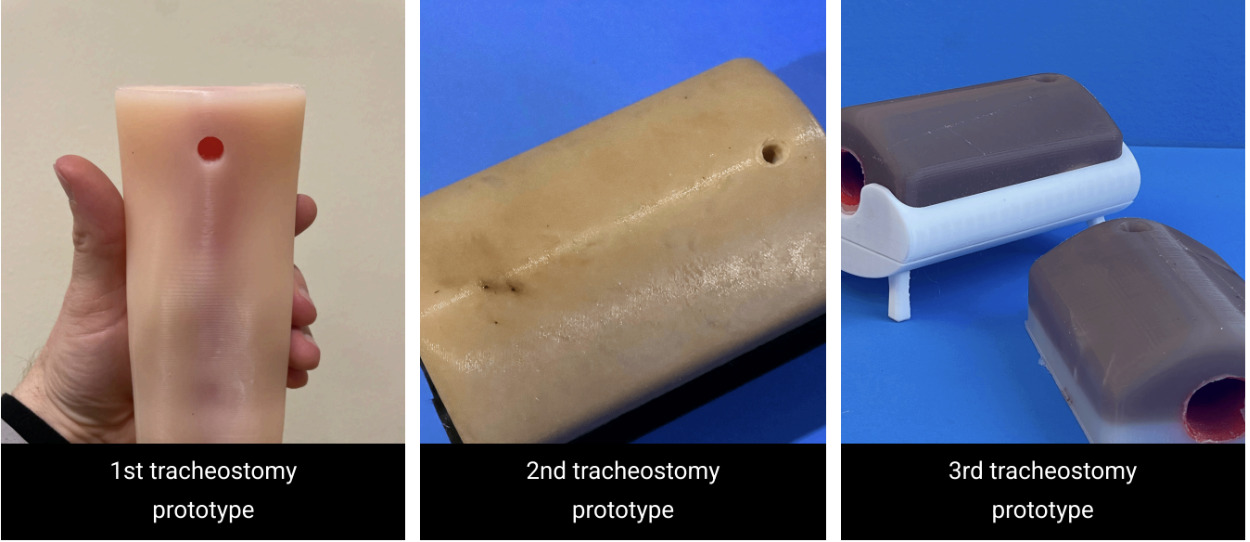
3D-Printed Model Development and Cost
The tracheostomy simulation model was produced using cost-effective materials, with a total production cost of $136.50 total with a per unit cost of $32.22 (Table 2). The model incorporated thermoplastic polyurethane (TPU) for airway structures over-molded inside of casted silicone for soft tissue simulation, seated in a polylactic acid (PLA) base. Additionally, reusable tracheostomy tubes, straps, and suction catheters were gathered to supplement the model and not included in the final cost analysis (Table 2).
The design and fabrication process was informed by resources available through the UCSF Makers Lab Project Repository, which documents similar applications of 3D printing for medical simulation models and training tools in low-cost, resource-limited settings (Supplemental Material).
Expert Evaluation
Five local otolaryngologists evaluated the model’s anatomical accuracy, clinical relevance, procedural realism, and training utility (Table 3). The model received average expert ratings of 4.5-5 out of 5 across all domains. Feedback highlighted high anatomical fidelity and strong alignment with common clinical scenarios encountered by GPs in Rwanda. The model was noted for its affordability and practicality as a sustainable alternative to imported mannequins, with recommendations for minor durability refinements. Reviewers recommended minor durability refinements, including reinforcing high-stress areas around the stoma, improving the adhesion between the airway insert and silicone base, and considering replaceable silicone inserts at the tracheostomy site to extend the model’s lifespan with repeated use.
Training Impact on Knowledge, Skill, and Confidence
Pre- and post-training participant self-assessments demonstrated statistically significant improvements in knowledge, procedural skills, and confidence (Table 4). Pre-training surveys indicated limited prior exposure to tracheostomy care, with low baseline confidence and procedural skill levels reported, Knowledge scores increased from 53.3% to 68.4% (+15%, p<0.001). Confidence ratings across all management tasks improved substantially, with increases ranging from +2.11 to +2.59 points on a 5-point Likert scale (p<0.001).
Objective skills assessments, conducted through an independent review of participant-recorded simulation videos, confirmed significant procedural skill improvements. Notable increases were observed in tracheostomy removal/insertion technique (+2.55 points, p<0.001) and post-tracheostomy care (+2.90 points, p<0.001), which included essential tasks such as suctioning to confirm tube patency, appropriate placement and tensioning of tracheostomy ties, and application of a dressing beneath the tracheostomy flange.
*Simulation Curriculum Feasibility
*Participants rated the simulation-based training highly for its clinical relevance and practical utility (Table 4). The 3D-printed model’s affordability and procedural realism contributed to the program’s feasibility for continued use in low-resource environments. Feedback supported incorporating simulation-based ENT education into ongoing professional development curricula.
This simulation-based tracheostomy management curriculum, supported by a novel 3D-printed model, enhanced general practitioners’ knowledge, procedural skills, and confidence in airway management. Expert validation and participant feedback confirmed the model’s clinical utility, affordability, and adaptability.
Discussion
This study demonstrates that a novel, low-cost, anatomically realistic 3D-printed tracheostomy model, when paired with a structured curriculum and expert-led instruction, significantly improved general practitioner knowledge, perceived skill, and confidence in performing essential tracheostomy procedures. Feedback from local ENT providers confirmed the model’s anatomical accuracy and clinical relevance, while GPs reported that the simulation training was both applicable and impactful in preparing them for real-world clinical scenarios. GPs are a critical cadre of care providers across Rwanda, given the availability of fewer than 30 ENT subspecialists for a population of over 13 million people.16 Importantly, the success of this project depended not only on the physical model but also on the design and delivery of the accompanying curriculum. Structured instruction, deliberate practice, and expert coaching were essential to maximizing the educational benefit, underscoring that the model and the curriculum should be viewed as equally critical components of the intervention.
In the simulation literature, fidelity is conceptualized along a spectrum encompassing physical, functional, and psychological realism.17,18 While our model does not incorporate the physiologic feedback or advanced features of high-fidelity simulators, it provides a higher degree of anatomical fidelity than many improvised, low-cost trainers currently used in low-resource settings. Accordingly, it is best classified as a low-fidelity but high-anatomical fidelity, low-cost task trainer. While prior studies have explored the use of both high-fidelity mannequins and lower-fidelity task trainers for airway management training in LMICs, many of these models remain prohibitively expensive or lack anatomical realism.1,2,10 Existing low-fidelity, low-cost models are driven by local initiatives and resource constraints.19 These models facilitate skills improvement and confidence but often lack the anatomical accuracy needed for more formal skill acquisition and confidence building for GPs.20,21 On the other hand, high-fidelity, high-cost models offer greater anatomical detail and more comprehensive simulation capabilities but higher costs may make them inaccessible to a wider population of learners.22 In global health practice, low-fidelity trainers are often more practical due to their affordability, reproducibility, and ease of local implementation. Our project exemplifies how such models can be designed to balance realism with cost, offering a feasible, sustainable solution for procedure-based training in LMIC contexts.
Participants emphasized the importance of ongoing access to the model at their healthcare facilities for deliberate practice, particularly in remote district hospitals with limited ENT or anesthesia support. Prior literature has established that simulation-based learning is most effective when combined with structured instruction, deliberate practice, expert coaching, and opportunities for feedback.9,11 Moving forward, continuing to integrate this model with a comprehensive airway management curriculum, inclusive of didactic content, emergency algorithms, and coaching from experienced providers, will be critical to maximizing its educational impact and sustaining long-term competency gains.
Beyond formal training workshops, participants asked for permanent access to the model at their healthcare facilities for ongoing practice, particularly valuable in remote district hospitals with limited ENT or anesthesia support. Additionally, several providers highlighted the potential utility of the model for patient and caregiver education, offering a tangible tool to explain tracheostomy care procedures to families.23,24 Broader dissemination of the model, contingent on the affordability of local printing resources, could enhance airway management capacity not only for providers in training but also for community health education initiatives.
While this study demonstrates significant immediate improvements in knowledge, skills, and confidence following simulation training with the 3D-printed tracheostomy model, it does not assess long-term retention of these gains. It is well recognized that initial post-training improvements may diminish over time without ongoing practice or reinforcement. Future research should include longitudinal follow-up to evaluate the durability of skills and knowledge retention among general practitioners. Additionally, while the model showed strong expert validation and positive participant feedback, further studies could explore scalability across diverse healthcare settings and its impact on actual clinical outcomes. Importantly, capturing more formal user-centered feedback on prototype usability and suggestions for improving sustainability through open ended exit interviews would strengthen the model’s relevance and acceptability, particularly if the training program is repeated or scaled up in the future. Finally, the sample size was limited to GPs in Rwanda, and findings may not generalize fully to other contexts or healthcare systems.
Conclusion
This project demonstrates the value of a low-fidelity, high-anatomical fidelity, low-cost 3D-printed tracheostomy task trainer as part of a structured simulation curriculum for healthcare providers in resource-limited settings. When combined with deliberate practice, expert coaching, and curricular reinforcement, the model significantly improved GP knowledge, skills, and confidence in tracheostomy management. Its affordability and ability to be produced locally make it a practical and sustainable option for expanding airway management training capacity in LMICs. These findings highlight the potential of low-fidelity but anatomically realistic models to complement comprehensive training curricula, enhance clinical competencies, and improve the quality of care for patients requiring tracheostomy.
Corresponding Author Information
Nina Patel, MS, MPhil
University of California, San Francisco
Department of Otolaryngology, Head and Neck Surgery
Nina.patel2@ucsf.edu
480-295-9147
Acknowledgements
The authors would like to sincerely thank the UCSF Makers Lab for their invaluable support in the design, creation, and manufacturing of the innovative 3D-printed tracheostomy model used in this project. Their expertise, resources, and collaborative spirit were instrumental in developing a cost-effective, high-fidelity training tool tailored for use in low-resource settings. This initiative would not have been possible without the dedication and technical guidance provided by the Makers Lab team.
Funding
This project was supported in part by CHESA (Center for Health Equity in Surgery and Anesthesia) funding awarded to Dr. Gratien Tuyishimire.
Conflict of Interests
None
Author Contributions
NP: development of model, project design, data collection, data analysis, manuscript drafting, manuscript editing
KP: data collection, curriculum development, manuscript editing and revisions
GC: manuscript editing and revision, skills rubric development
SD: development and refinement of model, manuscript editing
JB, HN, AH, AK, DS: training instruction, model refinement, manuscript editing and revision
CN, IN, JN, DN, GN, EU: manuscript editing and revision
NM, JA, OM: manuscript editing and revision, curriculum and training coordination
MJX, GT: project design, model refinement, manuscript drafting, manuscript editing, project oversight