Introduction
Tracheostomy is commonly performed to provide a stable airway in patients requiring prolonged ventilatory support, airway protection, or long-term pulmonary hygiene. Selection of the appropriate tracheostomy tube type depends on the patient’s clinical condition and airway protection requirements. Cuffless tracheostomy tubes are generally preferred for long-term management when aspiration risk is low; however, cuffed tracheostomy tubes remain necessary in patients with impaired airway protection or significant neuromuscular dysfunction.1 Multiple sclerosis (MS) is a chronic inflammatory demyelinating disease of the central nervous system that may lead to progressive neuromuscular disability. Advanced disease may result in severe spasticity, contractures, respiratory muscle weakness, and bulbar dysfunction, all of which can complicate airway management and tracheostomy care.2–4
Malfunction of tracheostomy cuff systems can rapidly compromise airway protection. Emergency salvage techniques have been described for damaged endotracheal tube inflation lines, including insertion of a small-gauge intravenous cannula into the severed inflation tubing to permit reinflation of the cuff.5 However, similar reports involving tracheostomy tubes are extremely limited.
We report a unique case of an emergency caregiver-performed modification of a tracheostomy tube inflation system following accidental severing of the inflation line. This case highlights the challenges of home tracheostomy care in patients with severe neuromuscular disease and underscores the importance of caregiver preparedness in managing airway emergencies.
Patient Information
A 42-year-old male with a longstanding history of multiple sclerosis was diagnosed at age 17. The disease progressed significantly by age 25, resulting in severe neuromuscular impairment and locked-in syndrome requiring a surgical tracheostomy. The patient had no additional significant medical comorbidities. He resided at home with his parents, who served as his primary caregivers. Both caregivers had received training in basic tracheostomy care, including suctioning and routine management of the tracheostomy tube. Previous attempts to transition from a cuffed tracheostomy tube to a cuffless tube resulted in recurrent aspiration and oxygen desaturation. Consequently, long-term use of a cuffed tracheostomy tube was deemed clinically necessary.
Clinical Findings
Due to advanced MS, the patient exhibited severe spasticity and contractures involving all major joints, particularly the elbows and wrists. The wrists were fixed in a flexed position resting against the sternum. These contractures limited voluntary movement but increased the risk of inadvertent traction on the tracheostomy tubing and inflation line during coughing episodes or muscle spasms. Mobilization of the upper limbs required considerable caregiver effort. Despite requiring regular suctioning, the patient maintained adequate baseline respiratory function and was not oxygen dependent. Cuff pressure was intermittently reduced during the day to minimize tracheal mucosal pressure injury; however, complete cuff deflation was not possible due to the persistent risk of aspiration.
Diagnostic Assessment
Immediately after the inflation line was pulled from the pilot balloon, the caregiver noticed that the cuff was rapidly deflating. Based on previous experiences during cuffless tube trials, the caregiver anticipated imminent aspiration. Immediate replacement of the tracheostomy tube was not feasible because transportation to the hospital was not immediately available and ambulance transport would have involved significant delay. Additionally, the caregiver was alone at home and unable to safely transport the patient independently. Given the imminent risk of aspiration and lack of immediate medical assistance, the caregiver attempted to restore cuff function by modifying the damaged inflation line.
Intervention
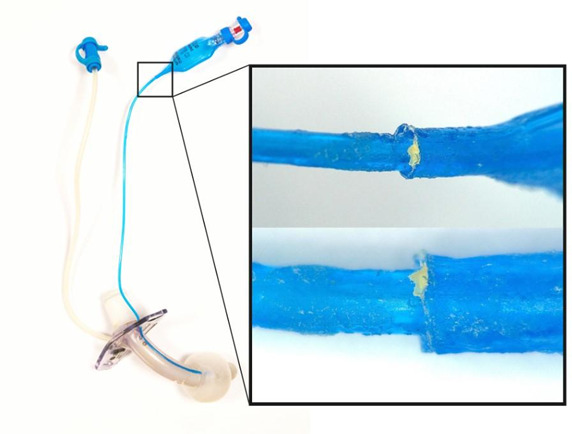
The caregiver trimmed the distal end of the severed inflation line using scissors to create a smooth, tapered edge. The modified inflation line was then carefully reinserted into the pilot balloon port. To secure the connection and prevent air leakage, the junction between the inflation line and pilot balloon was sealed with a small amount of cyanoacrylate-based adhesive (Figure 1). Care was taken to avoid occluding the lumen of the inflation line by inserting the tubing sufficiently deep into the pilot balloon before applying adhesive. Following the repair, the cuff was successfully reinflated to the desired pressure, restoring airway protection and preventing aspiration. Subsequent attempts by the authors to reproduce this repair using new tracheostomy tubes were unsuccessful.

Follow-Up and Outcomes
The improvised repair remained functional for four days. The tracheostomy team was notified on 1 July, and the tracheostomy tube was replaced on the same day. At the time of tube replacement, the patient showed no evidence of aspiration, infection, or airway complications. His clinical status remained consistent with baseline, and hospital admission was not required.
Case Discussion
Tracheostomy is commonly performed in patients with neuromuscular disease who require long-term airway access for pulmonary hygiene or airway protection. Clinical decision-making regarding tracheostomy tube type must consider the patient’s underlying pathology, swallowing function, and aspiration risk. While cuffless tracheostomy tubes are generally preferred for long-term management to reduce tracheal mucosal injury and facilitate speech and swallowing, cuffed tubes remain necessary in selected patients with impaired airway protection.6 In the present case, repeated attempts to transition to a cuffless tracheostomy tube resulted in aspiration and oxygen desaturation, necessitating continued use of a cuffed tube.
Advanced multiple sclerosis is associated with progressive neurological impairment that can significantly complicate airway management. Spasticity and joint contractures are common manifestations of advanced disease and may contribute to mechanical complications involving airway devices.7 In this patient, severe contractures of the upper extremities resulted in the wrists resting against the sternum, placing the tracheostomy cuff inflation line at increased risk of inadvertent traction during coughing or spasms. Respiratory dysfunction in patients with MS may also arise from respiratory muscle weakness, bulbar dysfunction, and impaired central respiratory control, all of which increase the clinical importance of maintaining effective airway protection.8
Malfunction of the tracheostomy cuff inflation system represents a potentially serious airway emergency because rapid cuff deflation may compromise airway protection and increase the risk of aspiration. Several salvage techniques have been described in the literature for damaged endotracheal tube inflation lines, including the insertion of a small-gauge intravenous cannula into the severed inflation tubing to enable reinflation of the cuff.5 However, similar reports involving tracheostomy tubes are extremely limited, and device modification is not recommended as standard practice.
This case highlights the complexity of decision-making in airway emergencies occurring outside of healthcare settings. At the time of the incident, the caregiver was faced with three potential management options: immediate tracheostomy tube replacement, awaiting medical assistance, or attempting restoration of cuff function through modification of the damaged inflation line. Each approach carried distinct risks. Immediate tube replacement outside of a controlled clinical environment may result in complications such as creation of a false tract, local hemorrhage, or loss of airway access, particularly in patients with longstanding tracheostomies or challenging anatomy. Conversely, delaying intervention while awaiting professional assistance could allow aspiration to occur following cuff deflation. The caregiver’s decision to attempt restoration of cuff function therefore represented a pragmatic risk–benefit assessment prioritizing rapid restoration of airway protection.
The successful reinflation of the cuff in this case was facilitated by the physical properties of cyanoacrylate adhesives. Cyanoacrylate compounds rapidly polymerize upon exposure to moisture through anionic polymerization, forming a strong adhesive bond within seconds.9 This property has led to their use in several medical applications, including wound closure and endovenous treatment of varicose veins.10 In this case, the adhesive effectively sealed the junction between the pilot balloon and inflation line, allowing the cuff to maintain pressure until formal tracheostomy tube replacement was performed. Despite this favorable outcome, cyanoacrylate exposure carries potential risks including dermatologic irritation, allergic reactions, and respiratory toxicity.11 Therefore, such modifications should not be considered routine practice.
The case also highlights broader considerations related to the structural integrity of tracheostomy devices. Tracheostomy tubes are commonly manufactured from polymeric materials such as polyvinyl chloride, silicone, or polyurethane.12 Prolonged exposure to respiratory secretions, humidity, and body temperature can contribute to gradual polymer degradation and reduced material durability.12–15 These factors may increase susceptibility to device malfunction over time, reinforcing the importance of adhering to recommended tracheostomy tube replacement intervals, as per European Union (EU) regulations.16
An additional important dimension of this case relates to the role of caregivers in the management of patients with long-term tracheostomies. Many patients with chronic neurological disease receive airway care primarily in home environments, where caregivers often develop significant experiential knowledge of airway management through repeated exposure to routine care and emergency scenarios. In this instance, the caregiver demonstrated a clear understanding of the functional role of the tracheostomy cuff and the potential consequences of cuff deflation. This situational awareness informed the rapid decision to attempt restoration of cuff function, which likely prevented aspiration and subsequent complications.
From a systems perspective, this case highlights the importance of structured caregiver education and emergency preparedness for patients managed with tracheostomies outside of hospital settings. Ideally, home tracheostomy care protocols should include the availability of spare tracheostomy tubes, caregiver training in emergency tube replacement, and clear escalation pathways for urgent clinical support. Simulation-based caregiver training programs may further enhance preparedness for rare but high-risk complications such as device malfunction.
Finally, this case raises broader considerations for airway device design and safety. Inflation line vulnerability represents a potential point of mechanical failure in tracheostomy systems, particularly in patients with limited mobility or involuntary movements. Future design improvements may consider enhanced reinforcement of inflation line junctions or protective configurations that reduce the risk of accidental traction.
Although modification of a tracheostomy device should not be considered standard practice, this case illustrates a rare scenario in which an improvised intervention restored airway protection in a time-critical emergency. The case provides valuable insights into airway emergency decision-making, caregiver expertise in home tracheostomy management, and the importance of preparedness for device-related complications. These lessons may inform future approaches to caregiver training, home airway safety protocols, and tracheostomy device design.
Conclusion
Self-modification of tracheostomy devices is not recommended and should not replace established emergency airway management practices. However, this case describes an extraordinary situation in which an improvised caregiver intervention restored tracheostomy cuff function and likely prevented aspiration. The case highlights several important considerations for patients with home tracheostomies:
-
Caregivers should receive comprehensive training in emergency tracheostomy management.
-
Spare tracheostomy tubes and essential equipment should always be readily available.
-
Routine tube replacement schedules should be maintained to minimize device deterioration.
-
Emergency plans should be clearly established for home-based airway complications.
Lessons Learned
-
Self-modification of a tracheostomy tube should be avoided except in extreme emergency circumstances when no alternatives are immediately available.
-
Caregivers of patients with long-term tracheostomies should be trained to recognize and respond to airway device failures.
-
Spare tracheostomy tubes and essential airway equipment should be readily available in the home setting.
-
Routine tracheostomy tube changes should be performed according to recommended schedules to minimize material degradation.
Caregiver’s Perspective
“I knew I had to act quickly because he was going to aspirate. We had seen this happen before when we tried cuffless tubes. I understood that the cuff needed to be inflated immediately to protect his airway.”
From the caregiver’s perspective, the decision to repair the device was made out of urgency and necessity. The caregiver’s familiarity with the tracheostomy system and prior experiences with cuff deflation and aspiration informed the rapid decision-making in this emergency situation.
Acknowledgements
The authors would like to thank the patient and family for their willingness to share their experience to contribute to clinical learning and improvement in tracheostomy care. Their cooperation and openness made this case report possible.
Ethical and Reporting Statement
This case report was conducted in accordance with the ethical standards of the authors’ institution and the principles outlined in the Declaration of Helsinki. Institutional review board approval was not required for a single-patient case report according to institutional policy. Verbal informed consent for publication of this case report. The manuscript was prepared in accordance with the CARE (CAse REport) reporting guidelines.
Conflicts of Interest
The authors declare that they have no conflicts of interest relevant to this manuscript.
Funding
No external funding was received for the preparation of this case report.
Authorship and Contributions (CRediT Taxonomy)
All authors meet accepted authorship criteria and approved the final manuscript. CJ.S contributed to conceptualization, investigation, data curation, and preparation of the original draft. L.D contributed to writing, review and editing, validation, and supervision. J.S contributed to writing, review and editing, and validation. JP.H contributed to supervision, writing, review and editing, and final approval of the manuscript. All authors agree to be accountable for all aspects of the work and ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding Author
Cornelius J Sauerman, MBChB
Department of Otolaryngology-Head and Neck Surgery, University Hospital Limerick, Dooradoyle, Limerick, Ireland
nellissauerman@gmail.com