Introduction
Tracheostomy is a common procedure to enable prolonged mechanical ventilation, bypass an upper airway obstruction, facilitate airway protection, and secretion clearance.1 Following insertion, timely and safe decannulation is a routine clinical goal.1–3 Intraoperative, early and late tracheostomy complications can occur, such as bleeding, infection, tracheal stenosis, and tracheomalacia,4,5 with approximately one quarter of patients experiencing at least one adverse event.6 Longer duration of tracheostomy cannulation increases the risk of tracheostomy-related adverse events, such as tube malposition and occlusion.7 Resource allocation and length of hospital admission are important considerations in patients with a tracheostomy, since health services may retain patients with a tracheostomy in an Intensive Care Unit environment to maximize patient safety.8,9
Timely decannulation maximizes patient comfort and often indicates improvement in medical stability and progress in the patient’s acute medical condition.10 As such, the timing and methodology of successful decannulation is of high interest. Several decannulation protocols and flowcharts have been proposed to optimize decannulation practice11–13; however no universally accepted method currently exists.14,15 Clinical steps within existing protocols and described practices usually include an assessment of the upper airway, such as placing a one-way valve, or capping the tracheostomy tube. A study involving tracheal manometry examined the differences in tracheal pressures in inflated and deflated tracheostomy cuffs, utilizing capping or one-way valves.16 One-way valve use has been well described as a facilitator of the assessment of upper airway function, restoration of voice and tolerance of this is a prerequisite for progression to decannulation in some studies.17,18 In 2014, Pandian et al developed a standardized capping and decannulation protocol,12 with the screening tool reportedly having 90% sensitivity and 100% positive predictive value for successful decannulation in fifty out of fifty-seven patients who were initially screened over a twelve-month period. In Nowak et al’s 2022 experimental study,19 the pressure drops in the trachea due to capping of the tracheostomy tube with a deflated cuff were equivalent to severe airway obstruction and resulted in a considerable increase in airway resistance. Tolerance of 24-hour capping has also been examined as an intervention to indicate readiness for decannulation compared with suctioning frequency while on continuous high-flow oxygen,20 in which high rates of capping trial failure were reported and were found to delay decannulation compared with the suctioning and high flow oxygen group. More research is warranted to guide standardized practice.
While decannulation is an important clinical goal, there exists a proportion of patients where decannulation is prolonged or not possible, and a long-term tracheostomy, with or without long-term mechanical ventilation is required. This is common in patients with neuromuscular diseases, such as spinal cord injury or Guillain-Barré syndrome. For this cohort of patients, clinical pathways should also incorporate interventions to improve quality of life, such as restoring communication options,21,22 and interventions that may facilitate discharge to the community, such as the use of non-invasive ventilation.23,24 Another indication for the need for different clinical pathways is the patient population where airway protection and/or airway patency are compromised but expected to improve in a timely fashion, without concomitant respiratory failure, such as in elective head and neck surgery or after stroke.
At Austin Health, multidisciplinary staff routinely assess and manage adult patients with tracheostomies in the Intensive Care Unit (ICU), with the Tracheostomy Review and Management Service (TRAMS) providing referral-based consultation as clinically indicated. TRAMS is a consultative multidisciplinary team, which routinely reviews and manages adult patients with tracheostomy from the inpatient wards and into the community.17 The team comprises respiratory physicians, clinical nurse consultants, speech pathologists, and physiotherapists. Austin Health is a quaternary metropolitan health service with state-wide services including the Victorian Spinal Cord Service and the Victorian Liver Transplant Unit as well as the Victorian Respiratory Support Service (VRSS), a home and virtual mechanical ventilation service that also supports the inpatient Ventilation Weaning Unit.23 Working collaboratively with TRAMS, these specialist services care for a complex cohort of patients, many of whom also require prolonged mechanical ventilation. Multidisciplinary team management of tracheostomy patients has been demonstrated to improve clinical outcomes, such as stepwise decannulation,24 emergency airway management,25 and early facilitation of communication.26
While these specialist multi-disciplinary tracheostomy and ventilation weaning teams have existed for over two decades, to date, local tracheostomy clinical pathways have not been formally described. This study aimed to examine the clinical characteristics of decannulated and non-decannulated patients, to inform the development of tracheostomy clinical pathways.
Materials and Methods
Retrospective cohort study
The first component was a retrospective observational cohort study design of patients who were decannulated and non-decannulated between January 2015 and December 2019. This time period was chosen due to the changes in clinical practice necessitated during the early years of the COVID-19 pandemic. Ethics approval was obtained from Austin Health Human Research Ethics committee (HREC/107394/Austin-2024) for the retrospective audit. The STROBE guidelines for observational studies guided the reporting of this study.27 Patient data was retrieved from the electronic medical record and the Global Tracheostomy Collaborative (GTC) database. The GTC database is a HIPAA compliant and meets applicable security and privacy standards, and was hosted on the REDCap web-based platform by Vanderbilt University during the study period. The GTC database contains administrative and process-of-care data for patients with a tracheostomy tube inserted during an admission (primary admission) and when a patient is admitted with a tracheostomy in situ (secondary admission), whether it be due to long-term tracheostomy or inter-hospital transfer.1,28 Data available in the GTC database include patient demographics, pre-tracheostomy insertion status and airway support, tracheostomy insertion, post-tracheostomy insertion status and airway support, clinical interventions to facilitate decannulation, tracheostomy tube changes, tracheostomy-related adverse events. GTC data accessed for this study was exported and analyzed by the study team. Descriptive statistics were calculated using means and percentages.
Consensus-based clinical pathway development
Classifications for weaning from mechanical ventilation have been described in the literature in the seminal work of the International Consensus Conference (ICC) on weaning from mechanical ventilation29 and more recently by The WIND study.30,31 These classifications define weaning success as the liberation from mechanical ventilatory support and the transition to spontaneous breathing. However, despite tracheostomy decannulation being an important clinical outcome, it is noteworthy that within the existing weaning definitions, tracheostomy decannulation is not a prerequisite for defining weaning success. Therefore, for this study, examination of the clinical characteristics of the cohort led to the development of two tracheostomy clinical pathways to reflect routine weaning practices that incorporate the existing weaning definitions and multi-disciplinary decision-making: 1) patients who were simple to wean from invasive mechanical ventilation (SW) who progress to decannulation, and 2) patients who require prolonged weaning from or long-term invasive mechanical ventilation (PW). An experienced multidisciplinary team was assembled to develop the clinical pathways. The team comprised respiratory physicians, an Intensive Care Specialist, physiotherapists, speech pathologists and a clinical nurse consultant (n = 10) who each had between 12 and 30 years of experience in tracheostomy care. Specialist expertise in the team ranged across critical care, complex head and neck surgery, respiratory medicine, chronic ventilation, neuromuscular diseases, and spinal cord injury.
Description of assessment and intervention components of the clinical pathways
Airway protection assessment and strategies
Airway protection in tracheostomy is an important consideration, with the aim of minimizing aspiration and optimizing safe decannulation. Comprehensive evaluation includes assessment of swallow function and above cuff secretions, cough strength, and laryngeal function, usually performed by a Speech Pathologist. Objective assessments, such as fiberoptic endoscopic evaluation of swallowing (FEES), are often utilized in conjunction with bedside swallow assessments.18,32 Strategies to facilitate airway protection include both non-pharmacological interventions; use of a Portex SuctionaidTM (Smiths Medical) port to aid above cuff secretion clearance, tracheal suctioning, patient positioning and swallow therapy17,26,33 and pharmacological approaches. Anticholinergic agents are commonly used to reduce secretion burden, particularly in patients with high aspiration risk or poor secretion management. Off-label use of atropine can be given sublingually and has been reported, particularly in acute or palliative settings where rapid reduction in secretions is required.34–36 These agents can support progression toward decannulation and reduce risk of aspiration; however, patients should be monitored for adverse effects such as dry mouth, tachycardia, sputum plugging from thickened respiratory secretions, and urinary or gastrointestinal issues.37,38
Airway patency assessment and strategies
Assessment of airway patency is essential to identify structural or functional obstructions prior to decannulation. Cuff deflation trials and one-way valve placement can facilitate clinical assessment of airflow through the upper airway, while endoscopic examination allows visualization of the supraglottic and glottic structures.11 Fiberoptic laryngoscopy is widely used to assess laryngeal function, airway diameter, and dynamic collapse during respiration.39,40 Strategies to improve airway patency may include modifying patient position, medical management of inflammation or edema, and surgical intervention when anatomical abnormalities are identified. Referral to Ear, Nose, and Throat-Head and Neck Surgery (ENT) is indicated if reduced airway patency is suspected, to assess for laryngeal pathology, laryngeal stenosis, vocal cord dysfunction, granulomas or persistent airway compromise.40,41 ENT involvement should be considered for individuals who are unable to tolerate one-way valve placement or present with dysphonia and/or stridor. Timeliness to identify and manage upper airway pathology can have a significant impact on successful decannulation.
Airway clearance assessment and strategies
Assessment of an individual’s capacity to clear respiratory secretions without requiring tracheal suction is a prerequisite for decannulation, particularly in those with a neuromuscular condition who may experience impaired airway clearance due to respiratory muscle weakness.42 Assessment should include i) volume of secretions, where high secretion load is a risk factor for decannulation failure, ii) cough strength, referring to the ability to clear secretions, which can be assessed by transit to the mouth when using a one-way valve or cap,42,43 or by measuring peak cough flow via the mouth, iii) ability to use cough augmentation strategies such as manual assisted coughing and mechanical in/exsufflation, if independent cough is insufficient44,45 and iv) lung volume, where higher lung volumes assist with the generation of higher peak cough flows secondary to elastic recoil of the chest wall.45
Decannulation: ward round, clinical documentation, pre- and post-observation procedure
At Austin Health decisions regarding the timing and appropriateness of ward-based decannulations are made by the consultative multidisciplinary tracheostomy service (TRAMS) in conjunction with the treating medical team. Where possible, these decannulations are ideally done within business hours between Monday and Thursday in the mornings, to allow increased observation.
Prior to decannulation, there is clear communication with appropriate ward staff and ICU medical emergency staff, and standardized documentation in the electronic medical record. This documentation denotes escalation plans in the event of acute deterioration, and clearly defined goals of care, specifically outlining the plan for reinsertion of the tracheostomy tube in the event of failed decannulation.
Post-decannulation observations are done half-hourly for the first two hours. Mandatory tracheostomy equipment46 remains at the bedside for forty-eight hours post-decannulation. If the patient exhibits stridor or respiratory distress post-decannulation, a rapid response team/medical emergency team (Respond Blue) is activated.
Decannulation to silicone stoma stent
Decannulation to a stoma stent can ameliorate the risk of decannulation failure in high-risk situations. Where the success of decannulation is uncertain, a stoma stent preserves the tracheostoma, enabling easy reinsertion of a tracheostomy tube at the bedside. Scenarios where stent use can be beneficial are in the presence of uncertain or dynamic upper airway patency and borderline respiratory insufficiency or cough strength.24
Decannulation to mini-tracheostomy tube
Insertion of a mini-tracheostomy tube into the tracheostoma, after removal of a standard tracheostomy tube, enables suction of tracheal secretions.47 The mini-tracheostomy tube is not an airway and does not provide airway protection but is solely for the purpose of secretion clearance. Although this product was used during the study period, it was unavailable at our institution at the time of manuscript preparation because it had been discontinued. In the absence of mini-tracheostomy availability, a 4mm tracheostomy tube can provide a similar level of support on the pathway to decannulation.
Communication interventions while invasively ventilated
Patients with a tracheostomy who are invasively ventilated or weaning from ventilation can utilize verbal and/or non-verbal communication interventions.48 Verbal communication interventions refer to those in which a patient uses their voice to communicate, for example, above cuff vocalization, ventilator-adjusted leak speech, one-way valve inline with the ventilator or while weaning off the ventilator.26,49 Non-verbal communication interventions refer to those in which a patient uses alternative and/or augmentative communication, also known as AAC, to communicate.50 Examples of non-verbal communication interventions which have demonstrated feasibility and utility in the ICU are eye gaze,51,52 electrolarynx,53 and communication boards.54,55 Patients who are critically ill and unstable in the early part of their ICU admission, may utilize AAC to communicate and proceed to verbal communication interventions as their respiratory function improves. A recent study found that patients who utilized AAC early in their admission had reduced tracheostomy cannulation time.7 Clinical trials of cuff deflation, assessment of secretion management and the assessment of upper airway patency assist in determining the most appropriate verbal communication intervention via the tracheostomy from the perspective of respiratory stability and communication effectiveness.26 Preliminary validation of the Communication with an Artificial airway Tool included both a clinician-reported scale and a patient-reported scale which are complementary in guiding selection of communication interventions and patient-centred rehabilitation programs for patients with a tracheostomy.56
Spontaneous breathing trial (weaning) practices
“Simple or short weaning” is defined as extubation after the first successful attempt of a spontaneous breathing trial (SBT) or the first attempt results in success within one day,28 while “difficult weaning” is defined as those who require up to 7 days to achieve successful weaning. For this study cohort, both “simple” and “difficult” weaning groups as defined by ICC29 or WIND30 criteria, largely followed the SW pathway. Prolonged weaning is defined as the need for at least three weaning attempts or required more than seven days of weaning after the first attempt29,30 and followed the PW pathway.
Non-invasive ventilation (NIV) practices
NIV has been described during the weaning process in patients with chronic critical care acquired weakness requiring prolonged mechanical ventilation.21,57 In this study cohort, the use of NIV is often considered following weaning from prolonged invasive mechanical ventilation in: a) patients deemed to be at high risk for failed decannulation and used prophylactically as a short-term therapy and b) patients likely to have ongoing nocturnal hypoventilation and chronic ventilatory failure, such as those with neuromuscular disorders or obesity hypoventilation syndrome.
Results
Clinical characteristics of the study cohort
In the study cohort of 440 patients, 323 (73%) were decannulated by hospital discharge. Most patients in both decannulated and not-decannulated groups were male (61% and 79% respectively). Age ranged from 16 to 90 years, with a similar mean age in both decannulated and not-decannulated groups (56 years and 59 years respectively) (Table 1). Patients admitted with respiratory or neurological conditions were most represented in the study sample. The most common reasons for tracheostomy insertion were for facilitation of ventilation or loss of upper airway patency.
Clinical and hospital outcomes
Clinical and hospital outcomes were examined, including length of hospital stay, duration of tracheostomy cannulation, survival to hospital discharge, and discharge destination (Table 2). Decannulation and survival rates were high (73% and 90% respectively). Almost all (95%) patients in the decannulated group survived to hospital discharge. Three quarters (76%) of the non-decannulated group survived; of these 72 (81%) were discharged with a long-term tracheostomy and 17 (19%) were discharged with a long-term tracheostomy and long-term invasive mechanical ventilation.
Tracheostomy clinical pathways
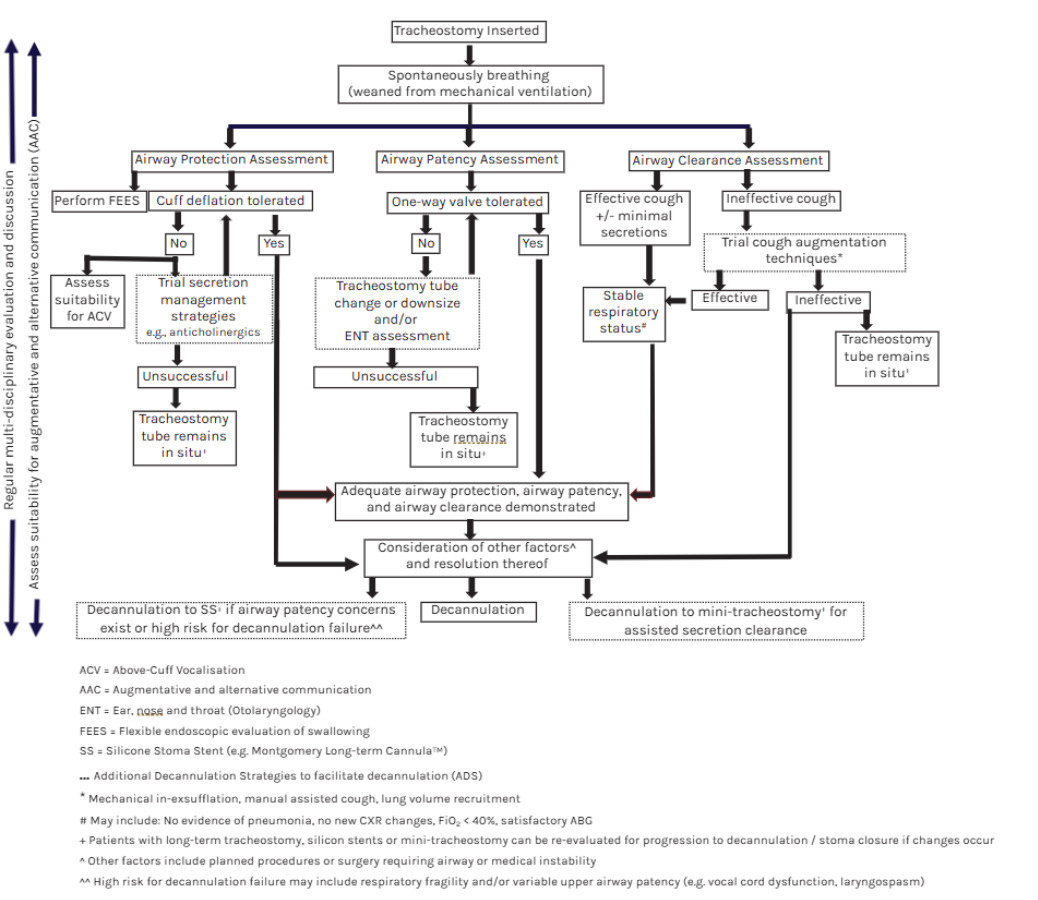
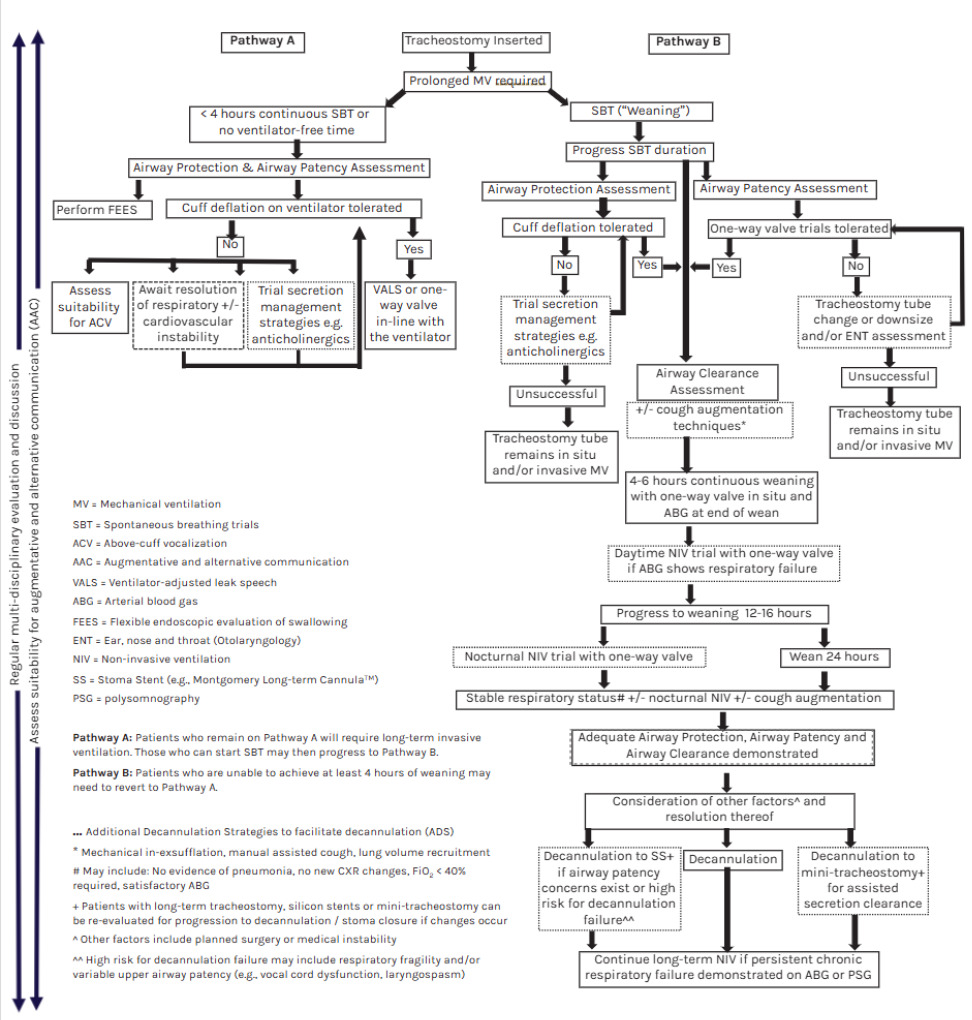
Two tracheostomy clinical pathways were developed by mapping the retrospective cohort data and the routine model of care at Austin Health. The first clinical pathway was developed for patients who are deemed simple or difficult to wean from invasive mechanical ventilation (SW) and progress to decannulation. The second clinical pathway was developed for patients requiring prolonged invasive mechanical ventilation (PW) which was comprised 2 tiers: 1) Unable to wean from invasive mechanical ventilation (<4 hours continuously or no ventilator-free time) and 2) Able to wean from invasive mechanical ventilation (Figures 1 and 2). Typically, patients with a head and neck primary admission were mapped to the SW pathway, where eighty-five percent of patients with a head and neck admission had a length of cannulation <20 days (range, 6-38 days). Patients of other clinical populations were mapped to either SW or PW pathways, with varied length of cannulation.
Each element of clinical practice within the tracheostomy clinical pathways is succinctly described. Elements of clinical practice within the simple to wean from invasive mechanical ventilation (SW) pathway include airway protection assessment and strategies, airway patency assessment and strategies, airway clearance assessment and strategies, communication interventions while invasively ventilated, and decannulation. Elements of clinical practice for patients requiring prolonged invasive mechanical ventilation (PW) include those elements from the SW pathway, with the addition of spontaneous breathing trial (weaning) practices, and non-invasive ventilation (NIV) practices. Additional decannulation strategies (ADS) were identified for both clinical pathways, including trial of secretion management strategies eg, anticholinergics; tracheostomy tube change or downsize, and/or ENT assessment; trial of cough augmentation techniques; decannulation to silicone stoma stent or decannulation to mini-tracheostomy.
_patients.png)
.png)
Discussion
Tracheostomy management and clinical decision-making regarding readiness for decannulation and weaning is complex. Duration of mechanical ventilation is one of the strongest predictors of function 1 year after critical illness58 and prolonged tracheostomy cannulation is associated with greater odds of experiencing a tracheostomy-related adverse event.7 Comprehensive and timely care requires an expert multidisciplinary approach which includes regular clinical evaluation, liaison, and communication across multiple treating teams and team members, including physiotherapy, speech pathology, nursing and medical.59 Standardized, evidence-based tracheostomy care with timely decision-making is required to progress respiratory weaning, restore communication and swallowing, and determine clinical suitability for decannulation. Patient care and the heterogeneous patient populations seen in a quaternary metropolitan health service require a multifaceted approach rather than a ‘one-size-fits-all’ protocol. The weaning practices, and additional decannulation strategies described in these clinical pathways provide a comprehensive approach to progressing ventilatory weaning and progression to decannulation. While these pathways are not validated nor prospectively tested, the two tracheostomy clinical pathways described are a visual and formal representation of the expert clinical practice developed and refined over the past two decades at Austin Health, across the continuum of care from the ICU into the community. There is notable value in the development of clinical pathways such as these, including standardisation of care and minimisation of unwarranted clinical variation, which can improve patient-centred outcomes, clinical outcomes, enhance safety and optimise resource utilisation.60
This retrospective clinical audit of tracheostomised patients admitted to Austin Health over the study period, highlighted a high decannulation rate (73% of all tracheostomy admissions) and high overall hospital survival rates (95% in the decannulated group and 76% in the non-decannulated group). With the support of specialist tracheostomy and home mechanical ventilation services, a high number of patients can be discharged into the community with long-term tracheostomy with or without ongoing invasive mechanical ventilation, either directly home, to an inpatient rehabilitation facility or a residential care facility. Pathway B within the PW clinical pathway is integrated with supporting evidence-based multidisciplinary procedures to maximise patient-focused outcomes, such as early communication restoration,18,26,61 weaning practices, airway clearance strategies, and cough augmentation techniques.62–65
Limitations
This study was a single-centre, retrospective study conducted in a quaternary hospital with dedicated tracheostomy and ventilation weaning services with mature processes and coordinated clinical practices. The results and entirety of the clinical pathways described here may not be generalizable or feasible in institutions with limited resources or expertise. However, it is the hope of the authors that dissemination of the information here enables recognition of the breadth of possible therapeutic options for patients with tracheostomy, thereby fostering collaboration within the clinical community. Potential strategies to improve patient care may include investment in skills development or strengthening referral pathways and partnerships with institutions with specialist teams.
These multi-faceted decannulation pathways are yet to be prospectively tested, though the authors are confident that the findings from the retrospective review of patient data are reflective of our routine clinical practice. Future direction will include the prospective testing of these pathways, to improve patient outcomes and timeliness of decannulation. Like all retrospectively designed studies, it is possible that missing data may have been omitted without the authors’ knowledge and therefore influence the overall results.
Conclusion
Two tracheostomy clinical pathways were developed to reflect the routine model of care in order to standardize approaches to anticipated rapid and prolonged mechanical ventilation weaning and tracheostomy decannulation. The complexity of this work reinforces the benefit of an experienced multidisciplinary approach. Robust programs of research are needed to strengthen the evidence in tracheostomy care globally. Future directions include prospective evaluation of these pathways, including the identification of determinants of necessity for prolonged ventilatory weaning in a heterogeneous population.
Conflict of interest
No conflicts of interest to declare.
Funding
No funding to declare.
Author contributions
CJZ - Conceptualization, Methodology, Formal analysis, Investigation, Data curation, Writing - Original draft, Writing - Review and editing, Project administration; CC - Conceptualization, Methodology, Formal analysis, Investigation, Data curation, Writing - Review and editing; JR - Conceptualization, Methodology, Writing - Review and editing; TC - Conceptualization, Writing - Review and editing; PG - Writing - Review and editing; CKC - Writing - Review and editing; MC - Writing - Review and editing; SW - Writing - Review and editing; NA - Writing - Review and editing; MEH - Conceptualization, Methodology, Writing - Review and editing, Supervision.
Corresponding author:
Charissa J Zaga
Department of Speech Pathology, Division of Allied Health, Austin Health
145 Studley Rd, Heidelberg, Victoria, 3084, Melbourne, Australia
E-mail: charissa.zaga@austin.org.au