Introduction
Intrahospital transport of critically ill adults, including those with surgical airways, is a common but high-risk component of modern hospital care. Surgical airways may take many forms, including tracheostomies, total laryngectomies, emergency cricothyroidotomies, laryngotracheal separations, and patients with stents or T-tubes that alter airway structure and require precise positioning. Although these surgical airways differ in anatomy and purpose, all create a direct conduit to the lower airway, and devices are often susceptible to dislodgement, malposition, obstruction, or loss of patency during movement. Transport heightens these risks because it occurs in less controlled environments with limited monitoring and personnel who may be unfamiliar with complex or nonstandard airway anatomy. For patients whose underlying medical conditions already increase vulnerability, even brief lapses in device function or recognition of airway compromise can lead to rapid deterioration, making transport hazardous without structured processes and trained teams. Although not all patients with tracheostomies are critically ill, this review focuses on transported patients with surgical airways who are typically hospitalized and mechanically ventilated, in whom the presence of a surgically created airway introduces transport specific risks distinct from those of critically ill patients without surgical airways.
Prospective work in mixed ICU populations shows that approximately one third of transports experience at least one mishap, often during transfers for CT or other procedures, despite stable pre-transport status.1 Subsequent studies have reported even higher event rates: in a Brazilian cohort of invasively ventilated patients, 67.2 percent of transports were complicated by clinically relevant cardiorespiratory alterations, and 75.7 percent had at least one adverse event related to equipment or personnel factors.2 Similarly, a Tunisian ICU audit found that 46.2 percent of transports were associated with mishaps, including oxygen desaturation, agitation, hemodynamic instability, accidental extubation, and cardiac arrest.3 Observational data from neurotrauma ICU transports show frequent technical events such as ventilator and monitoring disconnects, power failures, and interruptions in medication or drainage, with longer time outside the ICU and more infusion devices associated with higher mishap rates.4 Transport can cause device-specific vulnerabilities such as tube displacement, pressure injury, and interface-related complications, which are well documented among tracheostomy and intubated populations.5–9 Surgical airway patients are particularly vulnerable to airway loss and rapid physiologic deterioration, and institutional experience demonstrates that coordinated Difficult Airway Response Teams improve recognition and management of nonroutine airway emergencies.10–12
Beyond immediate physiologic instability, transport appears to amplify downstream infectious and resource burdens. In a prospective cohort of mechanically ventilated ICU patients, transport out of the ICU was associated with a fivefold higher crude incidence of ventilator-associated pneumonia (24.2 percent vs 4.4 percent), and transport remained an independent predictor of VAP after adjustment, alongside reintubation and tracheostomy.13 More recent work in a hyperbaric ICU population similarly identified intrahospital transport as an independent risk factor for VAP, with an adjusted odds ratio of 3.5 and associated increases in mechanical ventilation duration and ICU length of stay.14 In critically ill adult cancer patients, nearly one in three transports resulted in composite complications, including cardiopulmonary resuscitation, and events were significantly more common when patients spent more than 60 minutes outside the ICU.15
Evidence from pediatric and high-flow oxygen cohorts underscores that these risks are not confined to a single age group or ventilation modality. A systematic review of intrahospital transport in critically ill children found that physiologic deterioration, respiratory and airway complications, and even emergent tracheostomy and cardiac arrest occurred during transport, with many events judged preventable or mitigable through better preparation and checklists.16 In a recent multicenter study of adults on high-flow nasal cannula, clinically important complications still occurred during transport, reinforcing that the combination of critical illness and movement through the hospital remains hazardous even with more modern respiratory support strategies.
Despite these consistent signals of risk, the underlying processes of transport are poorly characterized, particularly for adults with surgical airways. Prior work in tracheostomy quality improvement demonstrates that standardized pathways, multidisciplinary teams, and protocolized care improve safety, reduce complications, and enhance efficiency in airway management.17–19 Most studies are single-center, heterogeneous in design, and rarely report granular details such as team composition, airway-specific monitoring, transport duration thresholds, or standardized handoff practices. Where process interventions have been studied, such as a partially structured operating room to ICU handoff protocol, significant reductions in information omissions have been demonstrated, suggesting that standardized communication can improve transitions for high-risk surgical patients.20 Expert guidance for ventilated adults emphasizes careful risk-benefit assessment, pre-transport stabilization, trained transport teams, and written policies specifying personnel, monitoring, and equipment requirements, yet implementation and evaluation of such recommendations for tracheostomy and other surgical airway patients remain limited.21
Intrahospital transport exposes critically ill patients to frequent physiologic instability, airway and respiratory complications, and increased infection risk, with potential downstream effects on length of stay and mortality.1–3,13–15 There is a critical gap in evidence-based guidance for safe transport within the hospital. The present scoping review therefore aims to map existing literature on intrahospital transport of adults with surgical airways, characterize reported complications and processes of care, and identify knowledge gaps to inform development of standardized, airway-focused transport protocols.
Methods
Eligibility criteria
This scoping review was conducted in accordance with the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines.22 We included primary research studies involving adults (≥18 years) with a tracheostomy who underwent intrahospital transport, defined as movement between locations within the same hospital for diagnostic, therapeutic, or procedural purposes. Eligible designs included randomized trials, prospective and retrospective cohort studies, observational audits, and interventional before and after studies. Comparators could include patients with versus without a surgical airway, pre versus post intervention groups, presence versus absence of a specialized transport team, or guideline-based versus usual care. Studies were required to report at least one outcome related to adverse events (accidental decannulation, airway obstruction, desaturation, cardiac arrest, mortality), efficiency (transport duration, therapy changes), or hospital utilization (ICU or hospital length of stay, readmission). We included English-language primary research with no date restrictions and excluded cadaveric or animal studies, interhospital transfers, dissertations, conference abstracts, reviews, guidelines, protocols, and case reports or case series.
Information sources and Search Strategy
A comprehensive search of six electronic databases was conducted on March 15, 2024. These databases included Ovid MEDLINE ALL, Embase Classic plus Embase, the Cochrane Central Register of Controlled Trials, the Cochrane Database of Systematic Reviews, CINAHL (EBSCOhost), and Web of Science Core Collection. The search strategy combined controlled vocabulary and free-text terms for surgical airways (for example, tracheostomy, tracheotomy, laryngectomy) and intrahospital transport (for example, patient transfer, which is movement between facilities or care levels, intrafacility transport, which is physical movement within the facility, and handoff, which is information sharing/communication during transfers and transports). Boolean and proximity operators were applied. Full search strings are provided in Supplementary Table 1.
Selection process
All search results were imported into Covidence,23 where duplicates were automatically removed. Two reviewers independently screened titles and abstracts using the eligibility criteria. Full texts were then reviewed in duplicate. Discrepancies at either stage were resolved by a third reviewer, and unresolved issues were adjudicated through team discussion.
Data collection process and Data Items
Two reviewers independently extracted data using a standardized form within Covidence. Extracted items included study characteristics such as design, country, study period, duration, and sample size; participant characteristics including age, sex, race when reported, comorbidities, and severity of illness scores such as APACHE II, SOFA, or Injury Severity Score; and transport-related variables such as type of surgical airway, indication for transport, duration or distance of transport, escort team composition, monitoring modalities, and equipment used. Outcomes extracted included adverse events, clinical instability, ventilator-associated pneumonia, resource utilization, and mortality. Missing data were recorded as “not provided,” and all discrepancies were resolved by consensus.
Study risk of bias assessment
Risk of bias for all non-randomized studies was evaluated independently by multiple reviewers using the ROBINS-I tool. Final judgments were reached through consensus.
Effect measures
Effect measures were extracted as reported by study authors. Continuous outcomes such as duration of mechanical ventilation and ICU length of stay were summarized using means or medians with measures of variability. Categorical outcomes such as adverse events, ventilator-associated pneumonia, and mortality were extracted as counts or proportions. P values were recorded when available.
Synthesis methods
Given heterogeneity in study designs and outcomes, results were synthesized narratively. Data were organized into structured tables and studies were arranged chronologically to facilitate comparison.
Certainty Assessment
Consistent with scoping review methodology, a formal certainty-of-evidence rating such as GRADE was not performed. Overall confidence in the evidence was informed qualitatively by ROBINS-I assessments, consistency of findings, and completeness of reporting.
Results
Study Selection
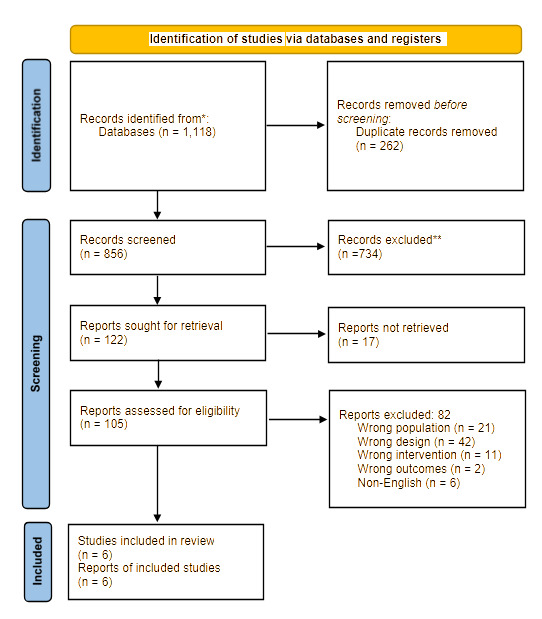
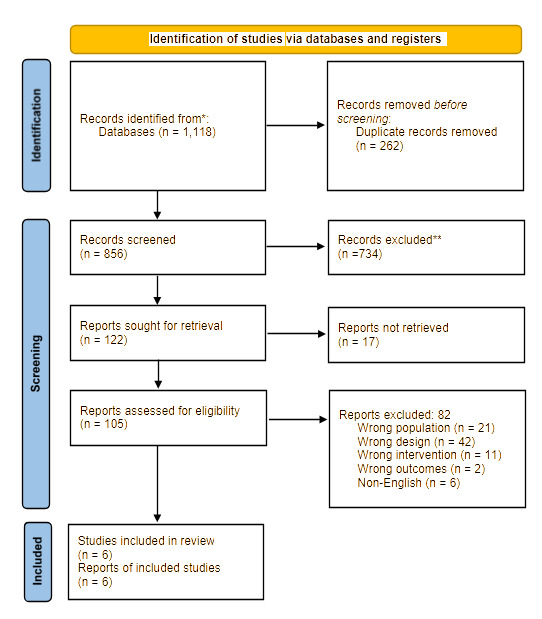
A total of 1,118 records were identified through database searching, of which 262 duplicates were removed, leaving 856 records for title and abstract screening (Figure 1). After screening, 734 records were excluded, and 122 full-text articles were assessed for eligibility. Seventeen full texts could not be retrieved, and 82 articles were excluded for reasons including wrong population (n = 21), wrong design (n = 42), wrong intervention (n = 11), wrong outcomes (n = 2), and non-English language (n = 6). Ultimately, six studies met the inclusion criteria and were included in the final analysis.
Study Characteristics
Six studies met inclusion criteria and varied in design, duration, and sample size (Table 1). Smith and colleagues conducted a prospective observational study in the United States over a 49-day period, capturing 125 intrahospital transports involving critically ill patients.1 Kollef and colleagues performed a large prospective cohort study of 521 mechanically ventilated ICU patients, although the study duration was not reported.13 A retrospective review by deBoisblanc and colleagues in the United States spanned 30 months and included 51 trauma patients undergoing weaning with bilevel ventilation.24 Zuchelo and Chiavone conducted a 20-month prospective observational non-randomized study in Brazil, evaluating 48 critically ill adults across 58 transports.2 Harish and colleagues performed a six-month prospective audit in India that included 120 critically ill cancer patients requiring transport out of the ICU.15 Lane-Fall and colleagues carried out a 36-month prospective interventional pre-post cohort study in the United States, examining 165 postoperative OR-to-ICU handoffs during implementation of a structured handoff protocol.20
Risk of Bias
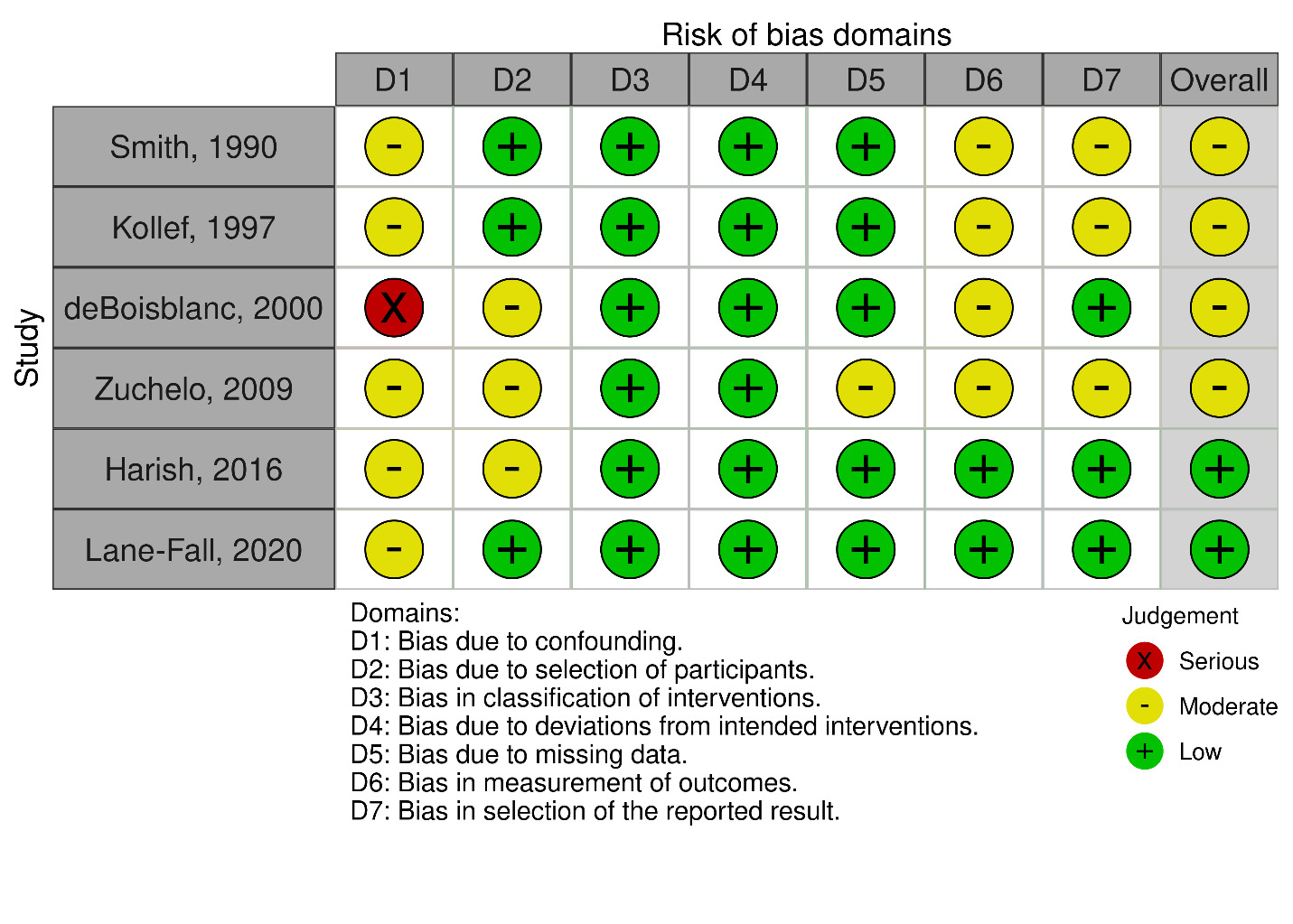
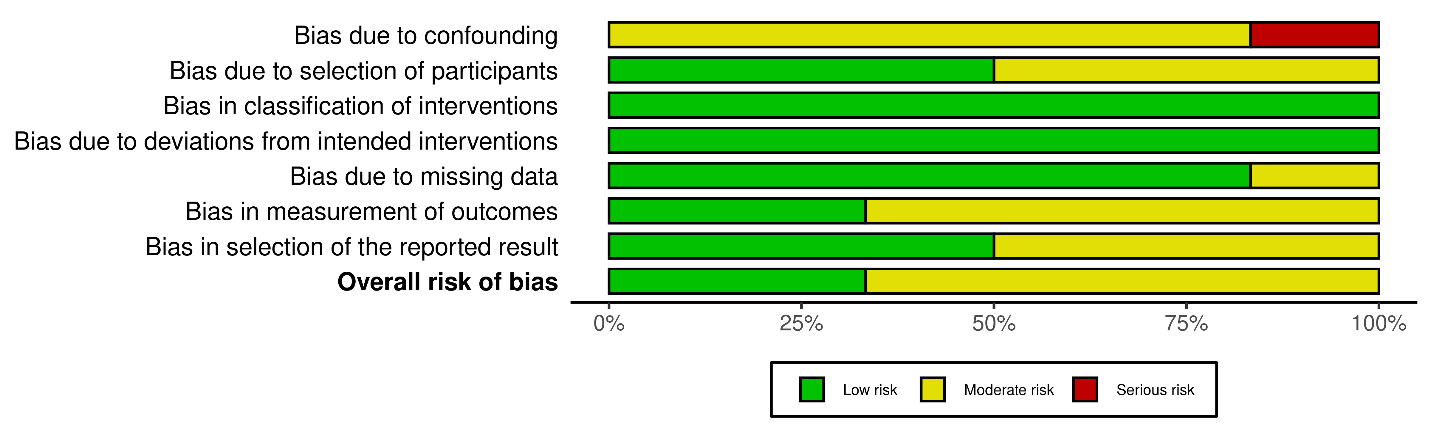
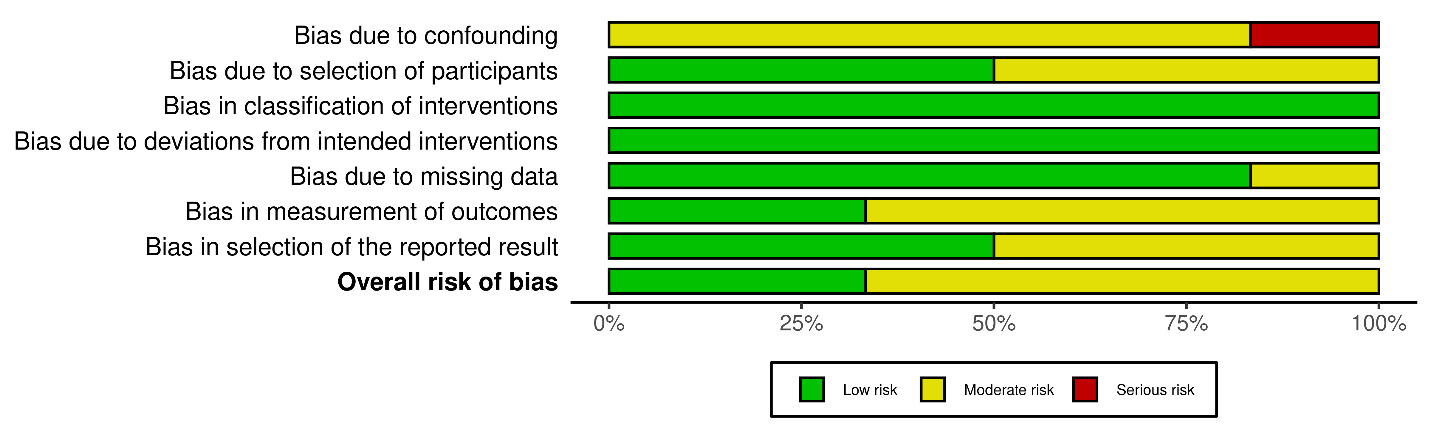
Risk of bias assessment using the ROBINS-I tool demonstrated that most studies had an overall moderate risk of bias across domains.1,2,13,15,20,24 All studies showed moderate risk in confounding due to their observational designs (Figures 2A & B). One study had a serious risk of bias in the confounding domain,24 although other domains were judged as low or moderate. Across studies, selection of participants, classification of interventions, deviations from intended interventions, and selection of reported results were generally rated as low risk, while missing data and outcome measurement were more commonly rated as moderate risk.

Participant Characteristics
Across the six studies, transported adult patients with surgical airways were generally middle-aged, with reported mean or median ages clustering in the early to mid-50s, reflecting a population with significant underlying illness severity (Table 2).2,13,15,24 When sex distribution was available, most cohorts were predominantly male, particularly among trauma and cancer populations.15,24 Racial and ethnic characteristics were largely unreported, with only one study providing demographic detail, showing a primarily White and Black patient population.13 Severity scores demonstrated consistently high acuity, including APACHE II values ranging from approximately 15 to 18 among mixed ICU cohorts, a mean Injury Severity Score near 30 among trauma patients, and elevated SOFA scores in cancer patients undergoing transport.1,2,15,24
Interventions
Important transport-related differences emerged across studies evaluating adults with surgical airways (Table 3). In a prospective ICU transport study, 43 of 125 transports (34.4 percent) involved at least one mishap, allowing comparison with the 82 stable transports to identify phases of transport and monitoring contexts most associated with instability.1 Among 521 mechanically ventilated ICU patients, transported individuals (n = 273) experienced significantly higher rates of ventilator-associated pneumonia compared with those who were not transported (n = 248), demonstrating a clear transport-related increase in infectious risk.13 In a trauma cohort, patients transferred to the surgical ward to complete bilevel weaning (n = 37) had longer ventilation durations compared with those weaned entirely in the ICU (n = 12), suggesting outcome differences based on weaning location.24 Physiologic instability during transport was frequent in a prospective Brazilian study, where 39 of 58 transports (67.2 percent) of mechanically ventilated adults exhibited cardiorespiratory alterations, including desaturation or hemodynamic changes.2 In critically ill cancer patients, transports lasting more than 60 minutes were associated with a substantially higher complication burden, with 18 events occurring in the >60-minute group compared with only 2 in the ≤60-minute group.15 A systems-level intervention study demonstrated process improvements, with postoperative surgical handoffs using a structured protocol showing fewer omitted information items compared with the pre-intervention group, indicating improved communication reliability.20
Clinical Outcomes Associated with Intrahospital Transport
Across studies evaluating intrahospital transport of adults with surgical airways or on invasive ventilation, transported patients consistently demonstrated worse clinical outcomes compared with non-transported groups (Table 4). In a large cohort of mechanically ventilated ICU patients, transport was associated with a notable increase in mechanical ventilation duration, with transported patients requiring an average of 8.5 ± 10.3 days compared with 2.3 ± 3.4 days among those who were not transported.13 ICU length of stay showed a similar pattern, with transported patients requiring 10.1 ± 10.7 days of ICU care compared with 3.4 ± 4.1 days for non-transported patients.13 Transport was also linked to increased hospital length of stay, with transported patients staying 18.1 ± 14.3 days compared with 10.6 ± 8.1 days in non-transported patients.13 Rates of ventilator-associated pneumonia were substantially higher among transported patients, occurring in 66 of 273 individuals (24.2 percent) compared with 11 of 248 individuals (4.4 percent) who were not transported.13 High rates of instability during transport were also observed in other studies, including cardiorespiratory alterations in 39 of 58 transports (67.2 percent) in a prospective study of mechanically ventilated adults2 and cardiac arrest in 20 of 120 critically ill cancer patients undergoing transport (16.7 percent).15 Mortality differences were reported in one comparative study, where transported ICU patients had a higher hospital mortality of 31.5 percent compared with 18.1 percent among non-transported patients.13 Other cohorts reported deaths during hospitalization but did not attribute them directly to transport events.1,15,24
Discussion
Intrahospital transport of critically ill adults with surgical airways appears both common and hazardous, with consistently high rates of physiologic instability, adverse events, and downstream complications across the limited studies identified in this scoping review.1,2,13,15,20,24 Transport was frequently associated with longer durations of mechanical ventilation, extended ICU and hospital stays, and higher rates of ventilator associated pneumonia, particularly among mechanically ventilated patients who left the ICU for diagnostic or therapeutic procedures.13,24 These findings suggest that intrahospital transport for adults with surgical airways are associated with preventable adverse events and should be approached as a high acuity intervention that demands structured preparation, team-based processes, and airway specific safeguards to mitigate preventable harm.1,15,21
Our findings align with other literature work in mixed ICU populations that has documented high rates of transport related mishaps, particularly in patients on invasive ventilation or vasoactive support.3,4,14 Prospective adult data indicate that cardiorespiratory alterations and equipment related events occur in up to two thirds of transports, and that longer time outside the ICU and greater infusion complexity increase the likelihood of adverse events, which is consistent with the patterns seen in the studies of ventilated surgical airway patients included in this review.2,4,15 The strong association between transport and ventilator associated pneumonia observed by Kollef and colleagues, and the identification of transport as an independent risk factor for VAP in a hyperbaric ICU cohort, reinforce the signal that movement through the hospital amplifies infection risk beyond baseline illness severity.13,14 Pediatric and high flow nasal cannula data further demonstrate that adverse events during transport, including emergent airway interventions and cardiac arrest, are not confined to traditional ventilator dependent populations and often appear preventable through better preparation and checklist use.16,25 What this scoping review adds is a focused synthesis of adults with surgical airways, highlighting the near absence of airway specific process measures in existing studies and the rarity of evaluations that explicitly address tracheostomy or laryngectomy patients as a distinct high risk group.1,2,15,24
Several findings emerging from this review merit particular attention for clinicians and health system leaders. First, the magnitude of difference in outcomes between transported and non-transported mechanically ventilated patients is striking, with approximately threefold longer ICU stays and fivefold higher crude VAP rates among transported patients in one large cohort.13 Second, the burden of acute instability during transport, including desaturation, hemodynamic compromise, and the need for cardiopulmonary resuscitation, underscores that these events represent not rare catastrophes but frequent features of routine hospital operations.1,2,15 Third, the absence of standardized protocols may contribute to a high rate of transport related complications. Therefore evidence tha a structured operating room to ICU handoff protocol reduces information omissions, even without immediate changes in mortality or length of stay, suggests that process standardization is both feasible and impactful in complex perioperative transitions.20 When viewed together, these observations argue that transport of adults with surgical airways should be conceptualized less as a simple logistic step and more as a vulnerable period in the continuum of critical care that is amenable to systems level intervention.15,21
Implications
The implications of these findings extend across education, practice, research, and policy. Educationally, interprofessional curricula for ICU, surgical, anesthesia, and ward teams should explicitly address intrahospital transport of patients with surgical airways, including risk recognition, equipment management, communication strategies, and contingency planning for accidental decannulation or rapid deterioration.16,21 In practice, institutions should consider developing airway focused transport pathways that specify minimum team composition, monitoring standards, and pre transport checklists for tracheostomy and laryngectomy patients, with particular attention to those receiving positive pressure ventilation or vasoactive support.1,2,15 From a research perspective, there is a clear need for multicenter observational cohorts and pragmatic trials that evaluate standardized bundles that combine risk assessment, sedation strategies, equipment checks, and structured handoffs for surgical airway patients undergoing transport.14,20 At the policy level, professional societies and accreditation bodies could support safety by articulating minimum expectations for intrahospital transport of high risk airway patients, including documentation standards, simulation based team training, and transport related quality metrics that can be tracked over time.16,21
Limitations
Several limitations of this QI project should be considered. First, although conducted as a scoping review using a comprehensive search strategy, only six studies met inclusion criteria, and most were single center observational designs with moderate risk of bias, which limits the ability to infer causality or generate precise effect estimates for transport related risk in adults with surgical airways.1,2,13,15,20,24 Second, reporting was heterogeneous and often incomplete, with many studies lacking surgical airway specific subgroups, detailed process measures such as escort composition or monitoring modalities, or consistent definitions of adverse events and outcomes, which constrained synthesis and precluded meta-analysis.1,2,14,15 Third, although the search strategy included terms for a range of surgical airways, including laryngectomy no eligible studies involving laryngectomy patients were identified. The lack of evidence therefore should be interpreted as a gap in the literature rather than an exclusion based on study design. Finally, this review was limited to English language publications and did not systematically capture grey literature or unpublished institutional protocols, introducing the possibility of publication bias and underestimation of both harms and effective mitigation strategies in this domain.16,22
Conclusion
Intrahospital transport of adults with surgical airways carries significant risk. These patients experience frequent physiologic instability, higher infectious and resource demands, and in some cohorts, increased mortality. Yet transport systems and protocols remain poorly defined and rarely evaluated. Multicenter prospective studies on transport that use standardized outcome measures for tracheostomy patients are needed. The absence of studies involving other surgical airway populations, such as laryngectomy, highlights a critical gap for future research. Studies should also test bundled approaches that combine pre-transport stabilization, airway-specific checklists, experienced transport teams, and structured handoffs. As health systems rely more on complex diagnostic and interventional pathways, there is value in developing defined protocols for transport of adults with surgical airways, incorporating careful preparation, skilled execution, and continuous quality improvement to ensure safe care.
Ethical & Reporting Statement
This scoping review involved analysis of previously published, de-identified data and did not involve human subjects. As such, institutional review board (IRB) review and informed consent were not required. The study was conducted and reported in accordance with the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines.
Conflicts of Interest
All authors declare that they have no conflicts of interest relevant to this work.
Funding
This work was supported by the Agency for Healthcare Research and Quality (AHRQ) through the Center for Immersive Learning and Digital Innovation: A Patient Safety Learning Lab advancing patient safety through design, systems engineering, and health services research (Grant R18HS029124; Principal Investigator: Vinciya Pandian). The funding agency had no role in the study design; data collection, analysis, or interpretation; manuscript preparation; or the decision to submit the manuscript for publication.
Authorship and Contributions
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship. VP and MJB conceived the study and provided overall supervision. NBG and IAS led the methodology, literature review, data extraction, and formal synthesis. NBG, NNSW, DMB, JRT, RS, YAG, SEH, FZG, AMF, LCN, LMW, and DG contributed to drafting the original manuscript. All authors participated in critical review, revision, and approval of the final manuscript and agree to be accountable for all aspects of the work.
Corresponding Author
Vinciya Pandian, PhD, MBA, MSN, ACNP, FCCM, FAANP, FAAN, FFNMRCSI
Associate Dean for Graduate Education and Professor of Nursing
Ross and Carol Nese College of Nursing, The Pennsylvania State University, University Park, PA
Department of Otolaryngology–Head and Neck Surgery, Penn State Milton S. Hershey Medical Center, Hershey, PA
Email: vpandian@psu.edu