Key points
-
Persistent and recurrent lower respiratory infections due to the colonization are common causes of hospitalizations for children with tracheostomy.
-
This paper presents a clinical suspicion that colonization and feeding/swallowing difficulties may pose a barrier to achieving successful decannulation.
-
The association between colonization and lower decannulation success may reflect subclinical or undiagnosed infection, as tracheostomized children often cannot demonstrate classic signs of respiratory infection, such as quantifiable increases in secretions.
-
Feeding and swallowing disorders may contribute to colonization, independent of tracheostomy duration, as microaspiration of gastric contents, aspiration of oral flora, and the presence of colonizing microorganisms can pose significant risks for pulmonary infection.
-
We emphasize the importance of factors that reduce the likelihood of decannulation for clinicians, especially in countries with limited resources and few multidisciplinary centers.
Introduction
Tracheostomy has become a significant health issue among children with medical complexity. The number of children undergoing tracheostomy and the accompanying chronic conditions has increased over the years, with a decrease in the age of the procedure.1–5
Decannulation should be considered in appropriate cases to minimise tracheostomy-related complications, improve the quality of life for the children and their caregivers, and reduce the health care costs.6
Successful decannulation rates in children range from 24 to 60%.2,7 However, an increased number of cumulative comorbidities lowers the chances of successful decannulation.8 Persistent and recurrent lower respiratory infections due to chronic identification of microorganisms are common causes of hospitalizations9–14 and significantly reduce the chances of achieving decannulation.15 Multidisciplinary pediatric centers are not widely available for children with medical complexity. The role of pediatrician and otolaringologist is critical in these settings.
In our study, we aimed to identify factors that may hinder successful decannulation. Our goal was to identify correctable factors to enhance the chances of achieving decannulation.
1. Material-Method
1.1. Patients
We retrospectively reviewed the medical records of pediatric patients with a tracheostomy at a tertiary hospital over seven years ending in 2019. Data including age, gender, underlying disease, presence of comorbidities, tracheal aspirate cultures, and home ventilation support post-tracheostomy were obtained from patient’s medical records. We compared differences between children who successfully decannulated and those who retained their tracheostomy.
Neurologic disorders (ND), congenital heart diseases (CHD), chronic pulmonary diseases (CPD), airway abnormalities, metabolic/genetic disorders were were categorized as the primary reasons for tracheostomy. Other associated conditions such as minor static neurologic disabilities and controlled epilepsy, hemodynamic stable structural heart defects and feeding and swallowing disorders were defined as comorbidies.
Feeding status of the children (tube feeding or oral feeding) and presence of feeding/swallowing disorders (which was defined as abnormal swallowing or respiratory symptoms associated with feeding) were also obtained from childrens’ medical records.
Tracheal aspirate cultures were obtained every three months during routine clinical visits regardless of any clinical signs of infection or any time with the presence of respiratory infections. The colonization was defined as the isolation of the same microorganism in more than 3 consecutive cultures of tracheal aspirate in continuous 12 months period without any respiratory tract infection (no fewer, no worsening dyspnea or no increase of aspirates, no chest infiltrates on radiography, no antimicrobial therapy).16
We included the results of tracheal aspirates from the last year before decannulation and for children who retained with tracheostomy, from the last year before December 2019, marking the end of the study period.
Statistical Analysis
The IBM SPSS Statistics (version 22.0 IBM Corp., Armonk, NY) software program was used to analyze the data. Categorical variables are presented as numbers (n) or percentages (%). Continuous variables are shown as medians with 25 and 75 percentages. For comparison; Mann Whitney u, Pearson’s chi-square test and Fisher’s exact tests were used as appropriate. A survival analysis (time to decannulation) was performed using a Cox proportional hazards regression model to determine predictors associated with time to decannulation. Variables from the univariate analyses with p values less than 0.05 were entered into the model. Predictors with hazard ratio exceeding a value of 1 indicate an increase in the chance of decannulation and hazard ratios lower than 1 indicate a decreased chance of decannulation. A p-value < 0.05 was considered significant for all comparisons.
1.2. Ethical Approval
The study was approved by the Ethical Committee of Medipol University Medical Faculty (Number: 10840098-604.01.01). Written informed consent was obtained from all parents/legal guardians before bronchoscopy and decannulation attempts.
2. Results
2.1. Clinical Demographics and Indications
We evaluated 171 tracheotomized children (54% male). Neurological disorders (49%), congenital heart diseases (17.5%), and airway abnormalities (11.7%) were the most common primary disorders among children with a tracheostomy.
Decannulation was successfully achieved in 59 children (34.5%), with a median age at decannulation of 22 months. The mean duration of tracheostomy was 46.7(±3.1) and 17.6(±1.8) months in children who remained with tracheostomy and those decannulated, respectively (Table 1). At decannulation, 24 % of children were under 1 year old, while 55% of them were under two years old.
Among the children, 82 (48%) required home ventilation support post-tracheostomy. Of these, 23 (28%) were decannulated. During the follow-up period, 16 of these children were liberated from the ventilator before decannulation. The remaining 7 children (3 with congenital central hypoventilation, 3 with spinal musculary atrophy type 1, and 1 with severe airway malacia) were decannulated with non-invasive ventilation (NIV) support.
Although primary ND or presence of a concomitant neurological comorbidities, in addition to other primary diseases, were associated with lower decannulation rates, one-third of them could still be decannulated. The primary reason for children being ventilator-dependent at discharge was attributed to the substantial number of children with neurological disorders (p<0.001).
Two (3.3%) children required tracheostomy replacement in 24-72 hours following decannulation due to decompansation of underlying cardiologic disease. In both cases, bronchoscopy prior to decannulation showed adequate airway patency. These patients were clinically more stable than the cohort in whom decannulation was not attempted, but later demonstrated transient decompensation related to underlying cardiac disease rather than airway obstruction.
2.2. Risk Factors Associated with Decannulation
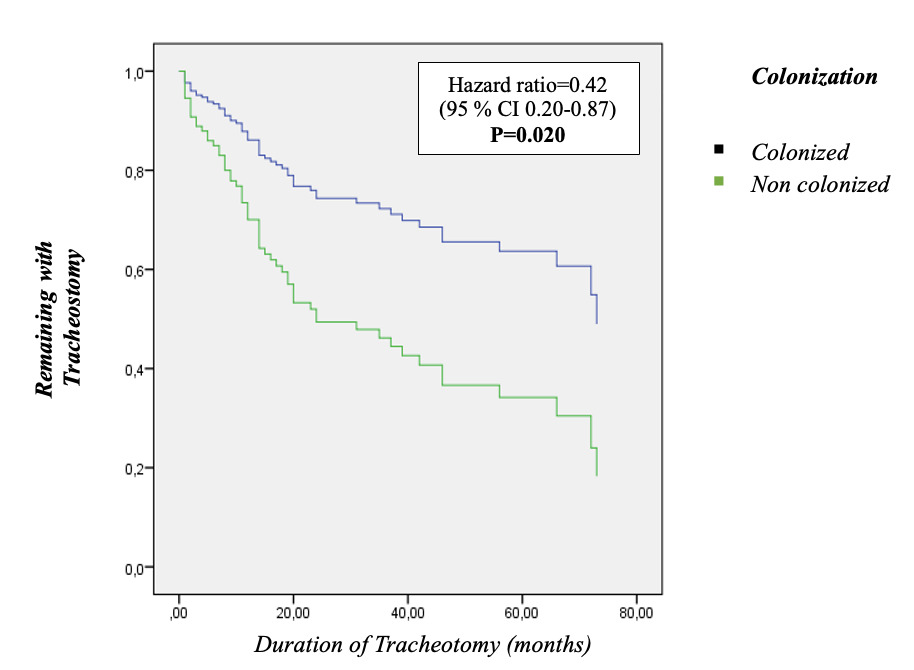
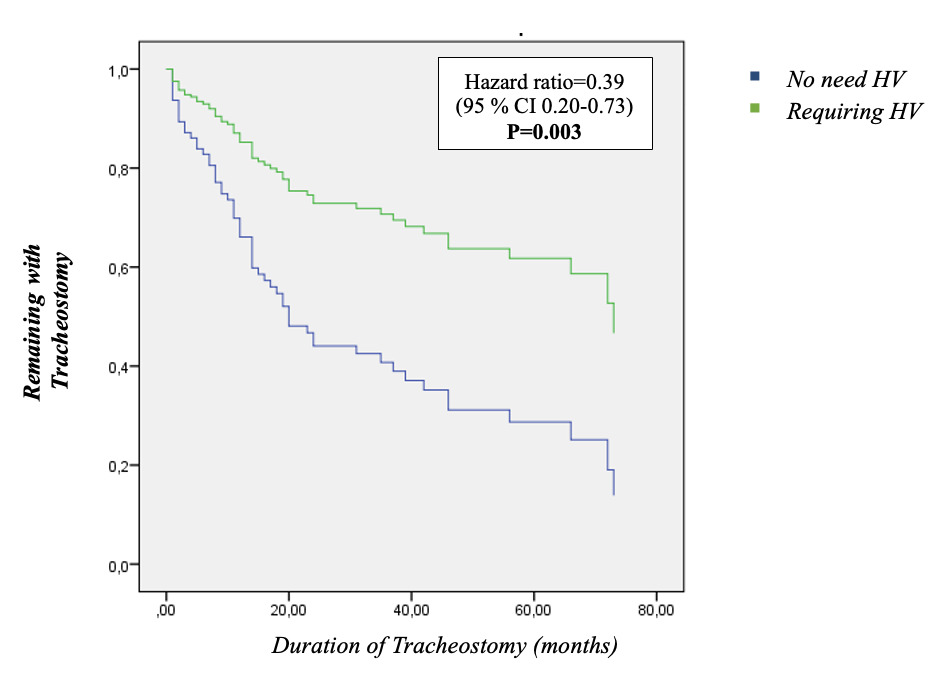
Multivariate Cox regression analysis revealed factors associated with decannulation (Table 2). Colonization (2.4-fold) and a history of home ventilation support post-tracheostomy (2.6-fold) were significantly associated with lower rates of decannulation. (Figure 1 and Figure 2).


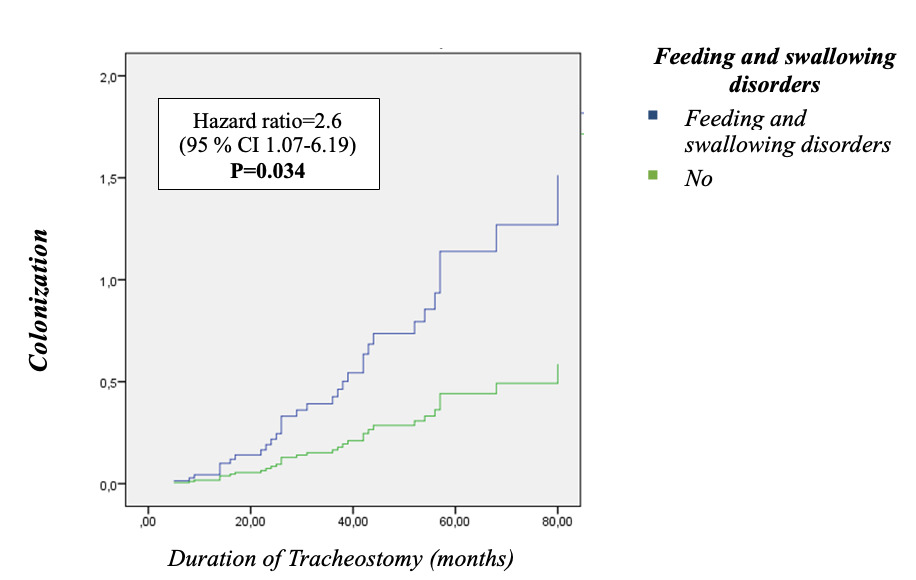
Colonization was present in 56 (33%) children with, Pseudomonas aeruginosa (60 %) and Staphylococcus aureus (13%) were the most commonly identified pathogens. Colonization was significantly more frequent in children who remained with a tracheostomy (p < 0.001), had underlying neurological disorders (p =0.002), required invasive respiratory support post-tracheostomy placement (p < 0.001), and experienced dysphagia or feeding disorders (p=0.002). There was a significant correlation between duration of tracheostomy and colonization (p=0.008). Having only feeding and swallowing disorders (2.6-fold) was identified as an independent risk factors of the colonization following the Cox regression analysis (Table 3 and Figure 3).

Mortality
No patients who were decannulated died and eighteen subjects (11%) died before the end of the study.
3. Discussion
Decannulation under safe circumstances should be considered in all children when the initial indication is no longer exists. Determination of the factors that decrease the possibility of decannulation is important for identify the targets that require attention. There have been few studies evaluating the clinical factors affecting the decannulation rate with big variations in terms of sample size and underlying conditions.15,17–20
Our study showed that colonization and invasive ventilation requirement following tracheostomy placement may have a negative impact on achiving decannulation. The presence of the colonization reduces the odds of decannulation rate by 2.4-fold, regardless of tracheostomy duration or precense of an ND or, invasive ventilation requirement. Additionally, feeding and swallowing disorders are independently associated with colonization, irrespective of tracheostomy duration.
3.1. Indications
Indications of tracheostomy may vary according to the specialization of center and patient population. The most frequent tracheostomy indications were ND (49%) and CHD (18%) in our study. Over the last 30 years,7 the indications for pediatric tracheostomy have shifted towards prolonged ventilation dependency,7 and the most frequent indications are neurological (% 39-51) and cardiological diseases (% 21-34) in large pediatric series.2,4 Children with complex medical issues often undergo tracheostomy during prolonged intensive care stays, yet they require follow-up in multidisciplinary clinics to mitigate underlying causes and comorbidities.
3.2. Factors Associated with Decannulation
In our study, 59 children (34.5%) were decannulated, with a median tracheostomy duration of 12 months. These results align with the literature, where decannulation rates range from 24 -60 %.2,3,7 The presence of genetic abnormalities, gastroesophageal reflux, dysphagia, and the absence of a multidisciplinary team follow-up were the main factors for decannulation failure; 17–20.
Our findings suggest that colonization may influence the decannulation success in addition to invasive ventilation requirement following tracheostomy placement.
Colonization
Colonization is a common problem in children with a tracheostomy, and the rate was 33% in our study. Pseudomonas aeruginosa was the most frequently identified pathogen (60%), consistent with previous studies.19,21–23 Elimination of natural protective effect of the upper airways, altered anatomy and recurrent aspiration of airway secretion may lead to chronic colonization and subsequent infections.16,24 In children with a tracheostomy persistent detection of Pseudomonas aeruginosa in tracheal aspirate cultures is known to increase the risk of pulmonary exacerbations10 and associated with worse clinical outcomes. This includes an increase the number of hospitalizations, length of stay in intensive care unit11 and lower probability of decannulation.15
Our study shows an association between the presence of feeding/swallowing disorders, respiratory support requirement following tracheostomy placement, concomitant neurological disorders, duration of tracheostomy, and colonization. Feeding/swallowing disorders (2.6-fold) were independent risk factor of colonization regardless of tracheostomy duration or ND or invasive ventilation requirement. Aspiration of the gastric contents, upper airway secretions and food into airways may cause airway inflammation, facilitate the colonization of the airways with pathogenic bacteria which may lead to lower respiratory tract infections and bronchiectasis.22–25 Also feeding dysfunction decreased the odds of a successful first decannulation attempt (5.5-fold) and cause decannulation failure.17 Swallowing evaluation has become crucial in the preparatory stages of decannulation and has been integrated into decannulation protocols due to its impact on decision-making processes and decannulation success.26,27
The presence of the colonization was found to decrease the odds of decannulation by 2.4-fold -irrespective of tracheostomy duration-, the presence of an ND, or invasive ventilation requirement by cox regression analysis. It may also increase the risk of hospitalization and the requirement for respiratory support, potentially impacting decannulation success inversely. Trachesotomy children get regular infections with increase secretions and varying symptoms which may or may not be treated with antibiotics. It can be difficult to determine where colonisation finishes and lower respiratory tract infection starts. Treatment of respiratory symptoms of patients with tracheostomy vary between clinicians.10,12,15,16,21 In our clinic we have a standard approach for treating respiratory symptoms. We do not consider as an infection unless there are signs of active infection such as fever> 38.4 °C, worsening dyspnea or increase of the tracheal aspirates and chest infiltrates on radiography. Active pulmonary disease was associated with lower likelihood of successful decannulation and with decannulation often not being attempted. Similarly, in our cohort, colonizations without respiratory symptoms was associated with reduced decannulation rates. In a recent published study conducted at our center, nebulized antibiotic treatment was shown to decrease the number of hospitalizations, reduce the length of stay in the intensive care unit, and the chronic identification of microorganism in symptomatic children with a tracheostomy.28 Clinicians in regions lacking specialized health centers for children with tracheostomy may consider monitoring children with feeding/swallowing disorders and tracheal aspirate cultures. Additionally, providing caregiver education on infection control measures could be beneficial. In our multicenter study, the ISPAT project (Implementation of a standardized training program for caregivers of children with tracheostomy), we demonstrated a decrease in hospitalization rates and emergency department admissions due to increased and/or color changes in secretions, as well as accidental tracheostomy complications.29,30
Invasive Ventilation Requirement Following Tracheostomy
Nearly half of our children (48%) required invasive ventilation following tracheostomy placement, which was associated with a 2.6-fold decrease in decannulation rates. In the literature, rates of the need for respiratory support in children with a tracheostomy ranged from 33-44%, with no observed correlation between the duration of respiratory support via tracheostomy and the decannulation rate.2,31,32
As reported in previous studies, the most common underlying disorder in children with tracheostomy was neurological disorders, consistent with our findings.2,3 Although primary ND or presence of a concomitant neurological comorbidities, in addition to other primary diseases, were associated with lower decannulation rates, one-third of them could still be decannulated in our population. Six of these children with ND were decannulated with non-invazive ventilation. In these children, residual ventilatory support was required predominantly during sleep or intercurrent infections. NIV-facilitated decannulation was performed only after confirming adequate airway patency and cough function, serving as a step-down approach to minimize tracheostomy-related morbidity.
3.3. Mortality
Children with tracheostomy have more frequent mortality rates which may be related with underlying disease (12.5-28 %) and preventible complications of tracheostomy (1-9%) itself.2,7,31,33 In our cohort 11% of children died, mortality was related to the underlying condition, and none of our decannulated patients died during study period.
4. Limitations
The retrospective design based on medical records was the main limitation of our study. Data on the type of tracheostomy tube (cuffed vs. uncuffed), standardized home ventilator cleaning, and changing the ventilator or tracheostomy cannula sets were not available before 2019.
We included children on ventilatory support in our analysis because they represent a clinically relevant subgroup in whom decannulation is still considered as part of long-term management. Excluding them might have limited the generalizability of our findings. Also the interval from liberation from home ventilation to decannulation attempt was not systematically recorded. Furthermore, based on this analysis, we have initiated a prospective study at our center entitled “Decannulation Success Following Aerodigestive Evaluation” to further investigate this subgroup.
5. Conclusion
The presence of the colonization may be associated with lower decannulation rates. Although the presence of the colonization rates naturally increase over time, their clinical significance is debatable. It is recommended that children with tracheostomy, particularly those with neurological disorder and/or swallowing dysfunction, should be followed-up regularly by clinicians for early detection of pulmonary parenchymal response. The presence of the colonization and feeding/swallowing problems should be investigated and caregiver should be trained for infection control measures.
Conflict of interest
The authors declare that they have no conflict of interest.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.