
INTRODUCTION
Acquired tracheoesophageal fistulas (TEFs) are rare but serious complications characterized by an abnormal connection between the trachea and esophagus. In adults, these fistulas are predominantly iatrogenic, often resulting from prolonged intubation, tracheostomy tube cuff overinflation, nasogastric tube use, or surgical trauma.1–4 TEFs can also arise from radiation therapy, chemotherapy, or esophageal stents.5–8 Symptoms typically include coughing during swallowing (Ono’s sign), recurrent pneumonia, persistent air leaks, and dysphagia, often appearing days to weeks after the inciting event.9,10 Early diagnosis and intervention are critical to preventing life-threatening complications such as aspiration pneumonia, sepsis, and airway obstruction.5
Diagnosis of TEFs relies on imaging modalities such as CT scans, flexible bronchoscopy, and esophagoscopy.5,11 However, small fistulas may go undetected with flexible bronchoscopy alone, necessitating the use of rigid esophagoscopy or insufflation for improved visualization.12,13 Treatment approaches range from conservative measures, such as repositioning the tracheostomy tube, to complex surgical repairs requiring interdisciplinary collaboration.14–16 Despite advancements, acquired TEFs remain challenging to manage, particularly in critically ill patients, due to high rates of morbidity and mortality.17,18
This report describes a complex case of dual mid-esophageal fistulas resulting from a combination of tracheostomy cuff overinflation and nasogastric tube trauma, highlighting diagnostic challenges, surgical intervention, and the impact of comorbidities on outcomes. The case is reported in accordance with the CARE (CAse REport) guidelines to ensure completeness and transparency in presenting clinical details.19
Patient Information
The patient was a 67-year-old woman with a medical history significant for hypertension, diabetes mellitus, and coronary artery disease. She presented with respiratory failure secondary to severe pneumonia, requiring mechanical ventilation. Her medical history also included a recent intracranial hemorrhage, for which she had been receiving inpatient care. At the time of admission, she was critically ill and unable to provide a detailed medical history, so her background was obtained from electronic medical records and family interviews.
The patient was initially managed with endotracheal intubation and ventilatory support. After 13 days of intubation, a percutaneous tracheostomy was performed to facilitate long-term respiratory management. During the procedure, the trachea at and below the tracheostomy site appeared normal. A Dobhoff tube was placed for enteral feeding, but the patient developed ileus, which delayed percutaneous endoscopic gastrostomy placement. A nasogastric tube was subsequently placed for gastric decompression.
During her hospitalization, she experienced multiple complications, including intermittent cuff leaks from the tracheostomy tube and increasing difficulty maintaining ventilatory pressures. These issues prompted multiple tracheostomy tube changes. Bronchoscopic and esophagoscopic evaluations were performed after clinical signs raised suspicion of a tracheoesophageal communication. The patient’s condition worsened over time, and additional comorbid factors, including prolonged mechanical ventilation and the presence of dual feeding tubes, were thought to have contributed to the eventual development of dual TEFs.
Her care was complicated by hemodynamic instability, requiring advanced decision-making among the multidisciplinary team and family. These discussions centered on risks versus benefits of surgical intervention and long-term prognosis given her critical condition and underlying comorbidities.
Clinical Findings
Key clinical signs observed during hospitalization included:
-
Ventilatory instability: Persistent air leaks through the tracheostomy tube, requiring escalating ventilator settings and frequent adjustments to cuff pressures to maintain oxygenation and ventilation.
-
Gastrointestinal dysfunction: Development of ileus following enteral feeding initiation, which delayed planned gastrostomy placement and necessitated nasogastric tube insertion for decompression.
-
Symptoms suggestive of tracheoesophageal communication: Coughing during Dobhoff feeding, increasing airway secretions, and suspected aspiration events indicated the potential for a fistula between the trachea and esophagus.
Timeline
Table 1 outlines the key events and their respective timelines in the clinical course of the patient, highlighting the progression from initial intubation to the eventual transition to comfort care.
Diagnostic Assessment
The diagnostic workup for this patient involved a multidisciplinary approach, incorporating imaging, endoscopic evaluations, and clinical correlations to confirm the presence of dual TEFs. The assessment was challenging due to the patient’s critical condition and the complexity of her presentation.
Initial Investigations:
- Clinical Indicators: Persistent cuff leaks, ventilatory instability, and coughing during feeding raised suspicion of tracheoesophageal communication. These signs prompted further evaluation to explore the integrity of the trachea and esophagus.
Definitive Diagnostics:
-
Flexible bronchoscopy revealed tracheal dilation and mucosal irritation near the tracheostomy cuff site, consistent with pressure necrosis. However, direct visualization of the fistulas from the tracheal lumen was challenging due to their posterior-lateral location and size.
-
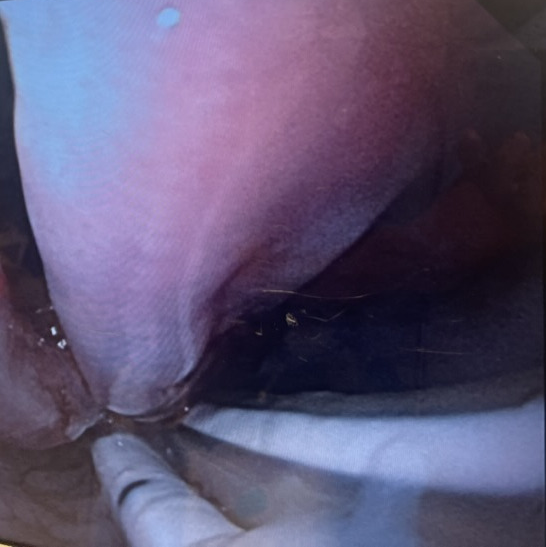
Flexible esophagoscopy initially suggested a mid-esophageal defect, but confirmation required rigid esophagoscopy with insufflation. This revealed two distinct tracheoesophageal fistulas, each approximately 4 cm in length, along the posterior-lateral tracheal wall (Figure 1).
-
Computed Tomography (CT) imaging performed postoperatively provided additional confirmation of tracheal cuff hyperinflation and its proximity to the fistulas. CT findings further highlighted the structural damage to the trachea and esophagus, correlating with the clinical suspicion of device-induced trauma.

Differential Diagnosis Considered:
-
Traumatic Injury from the Percutaneous Tracheostomy: Although possible, the timeline and location of the fistulas were more consistent with pressure necrosis from prolonged tracheostomy cuff overinflation against the two tubes within the esophagus.
-
Primary Esophageal Disease: No evidence of malignancy, strictures, or ulcerations was identified during esophagoscopy.
-
Iatrogenic Injury from Nasogastric Tube Placement: The presence of a nasogastric tube contributed to sustained pressure along the esophageal wall, potentially exacerbating ischemic injury.
Diagnostic Challenges:
-
The critical condition of the patient limited the ability to perform advanced diagnostic techniques such as barium swallow or dynamic imaging studies.
-
Small fistulas and their posterior-lateral location made direct visualization difficult with standard flexible bronchoscopy, necessitating rigid endoscopic approaches.
Therapeutic Interventions
The therapeutic approach in this case was multifaceted, involving urgent interventions to stabilize the patient’s respiratory status, mitigate ongoing damage from the tracheoesophageal fistulas (TEFs), and ultimately repair the structural defects. The complexity of the patient’s condition required collaboration among critical care, otolaryngology, and cardiothoracic surgical teams.
1. Initial Stabilization
-
Tracheostomy Management: Recurrent tracheostomy cuff leaks prompted multiple tracheostomy tube changes. To minimize further damage, the tracheostomy was eventually replaced with a Bivona foam cuff tracheostomy tube, positioned distal to the fistulas using flexible bronchoscopy. This adjustment provided better sealing and reduced pressure on the damaged tracheal wall.
-
Nutritional Support: Enteral feeding via the nasogastric tube was discontinued due to the risk of exacerbating esophageal injury and aspiration. Parenteral nutrition was initiated to maintain caloric intake while preventing further strain on the esophagus.
2. Preoperative Planning
-
Multidisciplinary Decision-Making: A family conference was held with the intensive care unit team, cardiothoracic surgery, and otolaryngology teams to outline the risks and potential benefits of surgical intervention. Given the patient’s critical condition, comorbidities, and the complexity of the surgical repair, detailed discussions were necessary to establish goals of care.
-
Optimization for Surgery: Hemodynamic stabilization and ventilatory support were prioritized. High oxygen support and bronchodilator therapy were used to optimize respiratory function before surgery.
3. Surgical Intervention
-
Operative Approach: The patient underwent surgical repair via a median sternotomy. This approach was selected to provide adequate exposure for both tracheal and esophageal reconstruction. The key components of the surgery included:
-
Esophageal Repair: A rotational omohyoid muscle flap was mobilized and used to overlay the esophageal repair, providing structural support and promoting healing.
-
Tracheal Resection and Reconstruction: A three-ring segment of the damaged trachea was resected, and anastomosis was performed using interrupted sutures to maintain airway integrity.
-
-
Intraoperative Challenges: The patient experienced significant intraoperative instability, including hypoxia and hypotension requiring multiple rounds of cardiopulmonary resuscitation. Venovenous extracorporeal membrane oxygenation (ECMO) was initiated via cannulation in the left groin after arterial calcifications precluded venoarterial ECMO. This supported oxygenation during the procedure.
4. Postoperative Management
-
The patient showed initial clinical improvement, with stabilization of ventilatory parameters and reduced tracheal secretions. The repositioned tracheostomy tube effectively minimized pressure on the surgical repair sites.
-
Careful nutritional management was implemented, with total parenteral nutrition (TPN) provided to support healing while avoiding esophageal strain. Drain output was monitored closely for signs of surgical site complications.
-
Postoperative CT imaging illustrated the repaired tracheal and esophageal sites, demonstrating tissue edema and inflammation at the repair locations. The repositioned tracheostomy tube minimized pressure on the reconstructed tracheal segment, as shown in Figure 2A and 2B.
_imaging.png)
Complications
-
Esophageal Leak:
-
On postoperative day 4 (POD4), the patient developed an increase in chest JP drain output, which tested positive for amylase, indicating an esophageal leak. The leak was managed conservatively with drainage and continued TPN, resulting in gradual improvement over several days.
-
Endoscopic evaluation confirmed that the esophageal repair remained structurally intact despite the early leak, and no further surgical intervention was required.
-
-
Esophageal Bleeding:
-
On POD10, the patient developed significant upper gastrointestinal bleeding, evidenced by bright red blood from the tracheostomy and oral cavity. This complication was exacerbated by anticoagulation therapy required for ongoing ECMO support.
-
Esophagoscopy localized the bleeding to the esophageal repair site, but the patient’s critical condition precluded aggressive interventions. Blood transfusions were administered to manage anemia, but bleeding persisted intermittently.
-
Follow-Up and Outcomes
Over the following days, the patient’s respiratory status deteriorated despite ECMO and ventilatory support. Persistent esophageal bleeding and declining organ function contributed to her worsening condition. After discussions with the multidisciplinary team and family, the decision was made to transition to palliative care, prioritizing the patient’s comfort and dignity. ECMO was decannulated, and ventilatory support was withdrawn. The patient passed away peacefully shortly thereafter.
Discussion
This case highlights the complexity of managing acquired TEFs in critically ill patients, highlighting the interplay of risk factors, diagnostic challenges, and the limitations of therapeutic interventions. Dual TEFs, as observed in this patient, are exceedingly rare and typically result from prolonged mechanical ventilation, overinflated tracheostomy cuffs, or nasogastric tube pressure, all of which were present in this case.20,21
The formation of TEFs is primarily driven by ischemic necrosis caused by prolonged pressure from endotracheal or tracheostomy tubes and feeding devices. Overinflated tracheostomy cuffs, particularly in cases with insufficient monitoring, can lead to mucosal erosion, creating a pathway for fistula development.3 Similarly, nasogastric tubes exert sustained pressure on the esophageal wall, contributing to tissue ischemia and ulceration.22 In this patient, the combination of dual feeding tubes and cuff hyperinflation likely accelerated the development of mid-esophageal TEFs. Table 2 outlines the common causes of iatrogenic TEFs, emphasizing the mechanisms through which pressure necrosis, surgical complications, and other factors can lead to fistula formation.
Diagnosing TEFs in critically ill patients remains challenging due to nonspecific clinical symptoms, such as coughing during feeding, persistent air leaks, and recurrent aspiration pneumonia.11,12,14 These symptoms often overlap with other conditions in critically ill patients, complicating timely identification. Table 3 presents the common clinical presentations of TEFs, highlighting key symptoms and their diagnostic significance. Flexible bronchoscopy, while useful, may fail to detect small or posterior-lateral fistulas, necessitating more advanced techniques such as esophagoscopy with insufflation or rigid esophagoscopy.12,13 In this case, the diagnosis was confirmed through a combination of bronchoscopy and esophagoscopy, highlighting the importance of a multimodal diagnostic approach.
Management of acquired TEFs involves both stabilizing the patient and addressing the structural defect. Conservative measures, such as repositioning tracheostomy tubes and providing parenteral nutrition, aim to minimize ongoing damage and promote healing. Definitive treatment typically requires surgical repair, which may include tracheal resection and esophageal closure with tissue flaps to reinforce the repair site.7,8,13
In this case, the use of an omohyoid rotational flap and tracheal resection via median sternotomy was appropriate for the patient’s condition, aligning with best practices for surgical repair of benign TEFs.23 However, intraoperative challenges, including the need for ECMO support and repeated CPR, significantly increased the risk of postoperative complications. The development of an esophageal leak on POD4 and bleeding on POD10 during anticoagulation therapy further complicated recovery, demonstrating the fragility of repairs in patients with significant comorbidities and critical illness.
Despite surgical repair, mortality rates for TEF patients with significant comorbidities remain high. Studies have reported mortality rates ranging from 0% to 11% for benign TEFs in surgically treated patients, but this increases substantially in critically ill populations.6,8 Factors such as prolonged mechanical ventilation, anticoagulation for ECMO, and intraoperative instability likely contributed to the poor outcome in this case.
This case highlights the need for proactive measures to prevent TEF formation, particularly in patients requiring prolonged mechanical ventilation. Key strategies include:
-
Cuff Pressure Monitoring: Maintaining cuff pressures below 25 cmH₂O to prevent tracheal ischemia
-
Minimizing Feeding Tube Trauma: Limiting nasogastric tube use and ensuring proper positioning to reduce esophageal pressure
-
Early Recognition of Signs: Symptoms such as persistent cuff leaks and aspiration should prompt immediate evaluation for potential TEFs
While surgical repair remains the standard for treating TEFs, improving prevention and early detection is essential to reduce morbidity and mortality.
Patient Perspective
Due to the patient’s critical condition and subsequent passing, a patient or family perspective on the challenges of care was unavailable for inclusion.