
Introduction
In light of evidence supporting the benefits of early tracheostomy tube insertion1,2 an increasing number of patients in Intensive Care Units (ICUs) are receiving mechanical ventilation via a tracheostomy. This coupled with reduced use of sedation3–5 means that patients who are ventilated are often awake, but unable to communicate due to the presence of an inflated tracheostomy cuff within the trachea. This cuff prevents airflow through the upper respiratory tract, preventing speech.
The inability of ventilated patients to communicate effectively has been shown to have a significant impact on their mental health.6–12 In addition, ineffective communication has been shown to negatively impact on overall health outcomes13,14 and is one of the largest contributing factors to sentinel hospital events.14
Whilst there are a number of Augmentative and Alternative Communication options,15,16 these are often difficult for critically ill patients to use effectively, and are reported to result in frustration among patients due to their inefficiencies when compared to vocalisation.17–21 Therefore, a large proportion of patients who require mechanical ventilation do not have an effective means of communication.
Ventilator Associated Speech Methods
There are three commonly used Ventilator Associated Speech (VAS) methods that are described in detail elsewhere by Zaga et al,22 these are:
Above Cuff Voicing
Above Cuff Voicing (ACV) involves use of a suction port to deliver air above the tracheostomy cuff and through the glottis to enable speech. This intervention is appropriate for patients who cannot tolerate cuff deflation, as it does not require deflation of the cuff or changes to ventilatory settings. Select patients can safely achieve functional speech via ACV, and ACV has been shown to have the potential to improve secretion management.23–29 Poor secretion management may result in prolonged cannulation and undesirable pulmonary sequelae.30,31 The use of ACV may therefore have the potential to not only facilitate verbal communication, but also decannulation.
Ventilator Adjusted Leak Speech
Ventilator Adjusted Leak Speech (VALS) occurs when the tracheostomy cuff is deflated and air from the ventilator is directed up through the glottis. Ventilator Adjusted Leak Speech has been used to safely achieve functional verbal output in long-term ventilated patients.32–37 There is currently no published evidence regarding the safety or effectiveness of VALS when used with acutely unwell patients in the ICU. Despite this, VALS is anecdotally more widely used within Australian ICUs than in-line speaking valves due to perceptions that it is easier and safer to implement, as it does not necessitate alterations to the ventilator circuitry.22,38
In-line Speaking Valves
In-line speaking valves redirect air from the ventilator into the glottis. The Passy Muir Valve (PMV) is the most commonly used in-line speaking valve. In-line PMVs (when used with patients who can tolerate cuff deflation and have a patent upper airway) have the potential to improve access to verbal communication for critically unwell patients7,39–41; and are consistently shown to be safe and not to have deleterious effects on the process of weaning from mechanical ventilation, or to prolong ICU length of stay.41–44
There are currently no published studies that directly compare the safety and effectiveness of ACV, VALS and in-line PMVs within the ICU setting.
Despite: a) a growing evidence base that supports the use of both ACV and in-line PMVs in ICU, b) patient preference to be able to communicate verbally,17,18 and c) the known implications of ventilated patients not having an effective and efficient means of communication,6–14 consistent use of VAS methods within Australian ICUs remains variable.
Whilst the anecdotally limited acceptability of VAS methods amongst healthcare professionals is cited as one of the potential barriers to their widespread use,42–44 there is no published evidence to support this theory. Similarly, there exists no research regarding healthcare professionals’ perceptions of the barriers and facilitators to the use of VAS methods.
Knowledge Translation
Theoretical frameworks can be used to facilitate conceptualisation, understanding and measurement of factors that are known to impact upon Knowledge Translation (KT).45–47 These factors include the acceptability of interventions and the perceived barriers and facilitators to their use.48,49
Theoretical Framework of Acceptability
Acceptability reflects the extent to which healthcare professionals deem interventions to be appropriate or agreeable50; and is increasingly becoming a key consideration in the design and implementation of healthcare interventions.50 It is additionally key to the translation of research into practice, as it is purported to be linked to engagement with interventions.48,51,52
Historically, definitions of acceptability and the methods used to measure it have been highly variable and not informed by theory.50 This issue has been addressed by the Theoretical Framework of Acceptability (TFA).50 The TFA was developed with reference to theories that provide a foundation for defining, understanding and evaluating the complex factors that influence acceptability.50,53 The TFA is comprised of seven component constructs, namely: affective attitude, burden, ethicality, intervention coherence, opportunity costs, perceived effectiveness and self-efficacy.50
Theoretical Domains Framework
The Theoretical Domains Framework (TDF) was developed to enable the comprehensive and systematic consideration of the behavioural determinants that may influence the implementation of healthcare interventions.54 It synthesises thirty-three theories relevant to implementation-related behaviour into 14 domains that represent individual, socio-cultural and organisational barriers to and facilitators of implementation and behaviour change.54
When used in conjunction, the TFA and TDF facilitate the exploration of the acceptability of, and barriers and facilitators to the use of interventions such as VAS.
Aim
The aim of this study was to explore the perceptions of relevant healthcare professionals working within Intensive Care with regards to:
(i) The comparative and overall acceptability of three different VAS methods (ACV, VALS and in-line PMVs),
(ii) Perceived barriers to and facilitators of the use of three different VAS methods (ACV, VALS and in-line PMVs).
Methods
Ethical Considerations
Ethical approval for this study (Ethical Committee Number: H0024285) was provided by the University of Tasmania Human Research Ethics Committee, Hobart, Tasmania on 14 April 2021. The research was undertaken in a manner consistent with the Guideline for Good Clinical Practice (GCP).55
Study Design and Setting
The Checklist of Reporting of Survey Studies (CROSS) was used to guide this research.56 This cross-sectional study used an embedded mixed methods survey design to address the project aims in the context of a 23-bed mixed medical and surgical ICU. This ICU was based in a 500+ bed metropolitan teaching and tertiary hospital where VALS and in-line PMVs are not used, and ACV is used inconsistently. This study setting is thought to potentially be reflective of other settings experiencing challenges in embedding use of all appropriate VAS methods into routine practice.
Survey responses were received between November 2021 and September 2022. An extended data collection period was provided to facilitate an increased response rate, in the context of the increased workload experienced by ICU staff during the global COVID-19 pandemic.
Survey
Data were collected using a 35-question survey that utilised Likert and free-text response items and was comprised of four sections: i) an introduction, ii) demographics, iii) the generic TFA questionnaire (adapted as per the author’s guidance to include wording specific to the topic of interest),57 and iv) questions relating to the perceived existence of barriers and facilitators to the use of each of the VAS methods (Supplemental Digital Content (SDC), Ventilator Associated Speech Survey). Preceding survey questions relating to each VAS method was a brief explanation of each intervention and information regarding each method’s: i) effectiveness, ii) regime, iii) safety, and iv) cost. These explanations were accompanied by diagrams and videos illustrating the practical application of each intervention. Videos for all three interventions were sourced from the National Tracheostomy Safety Project.58 Question branching was used to direct participants to questions relating to either retrospective or prospective acceptability, based upon each participant’s prior experience with VAS method use.
The survey was amended based on feedback from relevant healthcare professionals who worked within the acute hospital setting, but outside the ICU (to avoid contamination).59 In response to the feedback, minor changes were made to improve readability. The survey was administered via a secure online survey platform (LimeSurvey) and was distributed by two administrative assistants (one in Allied Health, the other in ICU) via an email containing a link to the survey.
Participants
Data were collected from a self-selecting convenience sample of nurses, doctors, speech pathologists and physiotherapists who work within the ICU. These professions were selected, as they are all frequently involved in the implementation of VAS methods in other centres, and in the use of ACV at the study site. The survey was distributed electronically to all 168 relevant healthcare professionals who were working in the ICU at that time. Participants were required to provide informed consent prior to being granted access to the survey and were instructed to complete the survey only once. Once submitted, all responses were non-identifiable.
Data Analysis
Demographic and Acceptability Data
Raw survey data was transferred to Microsoft Excel for storage and to enable easy transfer to Jamovi (an open-source statistical analysis software program). The data was screened for instances where participants had provided consent to participate in the study but had not completed any item of the survey. These “non-responses” were removed from the data set.
A group overall score of acceptability was calculated for each VAS method by computing a total mean score from the 7 TFA component construct questions. This method was used in-line with guidance from the TFA questionnaire’s authors and literature that encourages researchers to calculate total mean scores for Likert items used in the context of a survey scale (such as the TFA questionnaire).57,60,61 Data were screened for adherence to test assumptions via use of Mauchly’s test of sphericity, and differences in acceptability between the three VAS methods were explored using a one-way repeated measures ANOVA. Paired t-tests were used to explore the significance of any differences identified.
The highest possible acceptability score was 5 (completely acceptable). Ventilator Associated Speech methods were deemed to be acceptable if they received overall acceptability scores of 3.25 and above, and unacceptable if they received overall acceptability scores of 2.75 and below.
Barriers and Facilitators Data
Free text responses were transferred to NVivo. NVivo is a licensed software program that can be used to manage, organise and visualise qualitative data. Qualitative data were analysed using Deductive Positivist Manifest Content Analysis.62 This approach was selected as it aligns with the first researcher’s world view, reflects the limited depth of meaning that can be achieved via collection of free text survey responses,63 and because it enabled systematic description and quantification of the barriers and facilitators to the use of VAS methods.64 Description and quantification of this data enabled the assignment of importance to each domain of the TDF via use of frequency count percentages. By categorising TDF constructs by importance, the researchers were more readily able to identify priority areas in which interventions to facilitate implementation of VAS methods may be targeted. Domains of the TDF that received five percent (5%) or more of the total responses relating to barriers or facilitators were deemed to be key components to be addressed as part of KT interventions.
A coding framework based on the TDF was arrived at via discussion between the researchers. Following familiarisation with the code book by both researchers, and discussion regarding the rules of coding, all free text data were chunked into Meaning Units by the first researcher.65 The only text that was not chunked were conjunction words (e.g. “and”) that did not add meaning.
Meaning Units were defined as any combination of words that created conceptually meaningful chunks of text. These could take the form of single words, phrases, sentences or multi-sentence statements.62 This ad hoc method of chunking text for coding was reflective of the nature of the data provided by participants. Whilst some participants drafted paragraphs, others were limited to single words or lists of words.
Inter-Coder Reliability
An assessment of Inter-Coder Reliability (ICR) was undertaken to assess the robustness of the coding framework used.65 Prior to coding for the purposes of examining ICR, joint coding of the free-text responses from three surveys was undertaken in line with the guidance provided by O’Connor and Joffe.65 Following this, independent coding of the entire sample by the first researcher was conducted. Following further discussion to clarify the coding rules, a sub-sample of free-text responses from approximately 10% (n=7) of the participants was independently coded by the second researcher. The participant responses used for ICR were randomly selected using an online random number generator.
There is no consistent guidance on how to report on the outcomes of ICR. Therefore, both percent agreement and Cohen’s Kappa were calculated and reported. Percent agreement over 70%66 and Cohen’s kappa over 0.6167 were deemed to indicate substantial agreement between the two researchers.
Results
Participants
Of the 168 eligible participants, 64 (38%) provided survey data. Of those 64, 45 (70.3%) were nurses, 14 (21.9%) were doctors, three (4.7%) were speech pathologists and two (3.1%) were physiotherapists. The sample grossly reflected the relative proportions of the nursing, medical and allied health workforces within the ICU at the time of survey distribution.
Questions relating to VALS and in-line PMVs were not completed by five and 10 participants (respectively). This non-response likely reflects the order in which questions regarding these procedures were presented (i.e., second and third respectively).
Inter-Coder Reliability
Cohen’s kappa and percent agreement for independent assignment of free text responses to the TDF domains were 0.75 and 96.5% respectively, indicating robustness of the coding framework used.
Acceptability
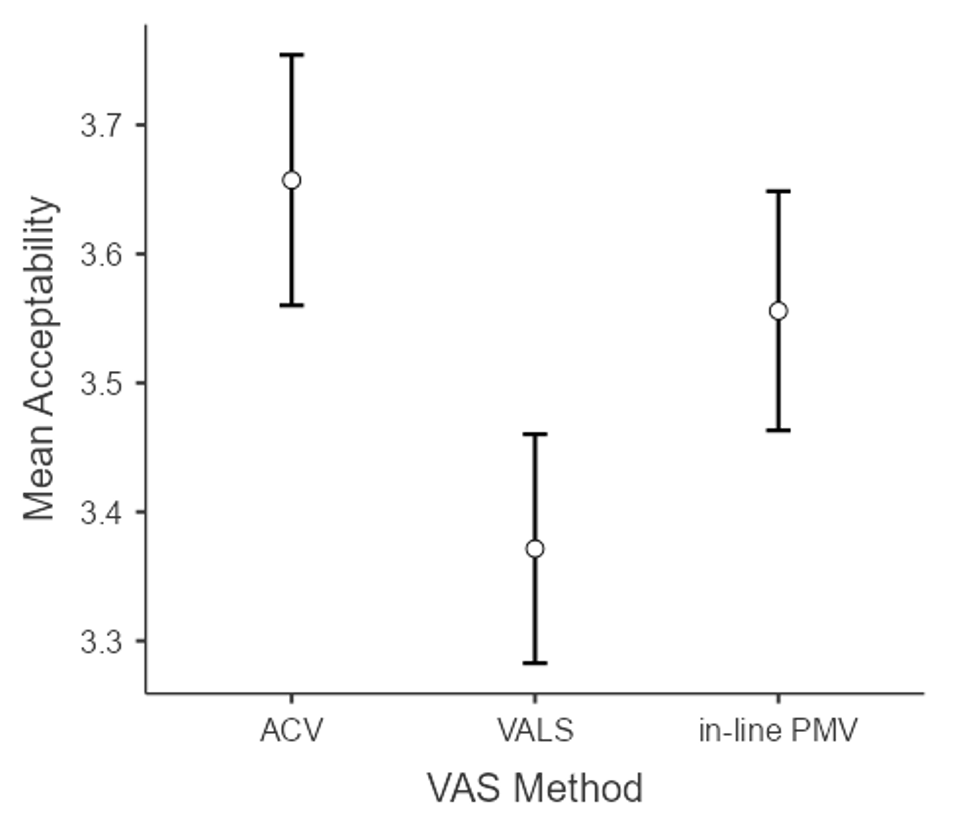
A one-way repeated measures ANOVA revealed that the perceived acceptability of VAS methods was influenced by VAS method type (F(2,108) = 16.0, p <.001, η²=.108).
Unadjusted post-hoc comparisons revealed that VALS (M=3.37, SD=0.33) was deemed to be significantly less acceptable than both ACV (M=3.66, SD=0.35, p<.001, d=0.75, 95% CI [0.46, 1.04]) and in-line PMVs (M=3.56, SD=0.34, p<.001, d=0.50, 95% CI [0.22, 0.78]) (see Figure 1). Both Cohen’s d results indicate a moderate effect size, suggesting practical significance.68
_methods_(error_bars_repr.png)
Barriers and Facilitators
A total of 268 Meaning Units related to the perceived barriers and facilitators to the use of VAS methods in ICU were coded to 13 of the 14 TDF domains. The only domain to which no Meaning Units were coded was “Optimism.” Comparatively more Meaning Units were coded as barriers (n=151) than facilitators (n=117) (see Figure 2).

The domains of the TDF to which five percent (5%) or more of the total Meaning Units for both barriers and facilitators were coded are identified in Tables 1 and 2; along with excerpts from survey responses that are illustrative of the free text responses received.
Management of Researcher Bias
The first researcher’s assumptions and expectations were monitored and challenged in regular discussions with the second researcher. It was found that some of the findings reported in this paper did not align with the first researcher’s expectations, suggesting adequate management of researcher bias.
Discussion
Acceptability
Whilst the anecdotally limited acceptability of VAS methods amongst healthcare professionals is cited as one of the primary barriers to their widespread use,42–44 ACV, VALS and in-line PMVs were all deemed to be acceptable by relevant healthcare professionals in the study facility. This finding raises a compelling question: if these interventions are deemed acceptable, why are they not being incorporated into routine practice?
Whilst it can be argued that intervention acceptability is essential to the successful and sustained implementation of new interventions,57 the acceptability results reported in this paper highlight that acceptability alone is not sufficient to facilitate the uptake of interventions.
Ventilator Adjusted Leak Speech was deemed to be significantly less acceptable than both ACV and in-line PMVs. As ACV is the only VAS method currently in use in the study setting, and PMVs are regularly used with patients not on ventilators in the study setting, this finding suggests that familiarity with interventions may have some impact upon their acceptability.
The finding that VALS was significantly less acceptable than in-line PMVs is noteworthy, as VALS is anecdotally more widely used within Australian ICUs than in-line PMVs. This is reportedly due to the perception that VALS is safer and easier to administer as it does not necessitate alterations to the ventilator circuitry.22,38 This poorer reported acceptability of VALS was supported by free text responses relating to the TDF domain of “Beliefs about Consequences”. Expressed concerns relating to the safety of VALS included the risk of aspiration, the potential for prolongation of ventilation time and the potential for lung derecruitment. Despite both VALS and in-line PMVs necessitating tracheostomy cuff deflation, the aforementioned concerns raised about VALS were not routinely reported in relation to the use of in-line PMVs for which there exists evidence regarding both its safety and effectiveness in Intensive Care.7,39–44 Evidence also exists regarding the low incidence of serious adverse events relating to ACV use in ICUs,69 suggesting that perceptions of intervention safety may have some impact on acceptability.
Barriers and Facilitators
The majority (i.e., eight out of 13) of TDF domains had both barriers and facilitators to the use of VAS methods mapped to them. “Environmental Context and Resources” was the domain to which facilitators were most frequently mapped; with access to skilled staff frequently cited as a facilitator. Conversely, inability to access skilled staff was frequently cited as a barrier to VAS use. “Beliefs about Consequences” was the domain to which the most barriers were mapped; with mention of concerns relating to the safety of interventions (predominantly VALS).
Knowledge Translation Interventions to Address Barriers and Leverage Facilitators
The key TDF domains to which reported barriers and facilitators were mapped were used to compose a theory-informed KT intervention plan.70 In light of the known importance of aligning KT objectives with evidence-practice gaps,49,70 as well as considering the relatively lower levels of acceptability among healthcare professionals regarding VALS, only ACV and in-line PMVs were chosen as the focus of KT interventions.
The intervention types, modes of delivery and content that make up the formulated KT plan (see Table 3) were selected based on guidance provided by Fahim et al70 in their theory-informed KT workbook. In formulating the KT plan, consideration was also given to the local context and the details of free text responses received relating to the barriers and facilitators to VAS use.49,70
In the context of current healthcare workforce shortages74 and driven by recognition that a shortage of resources, particularly staffing, was reported as a barrier to the successful implementation of VAS methods; it was deemed necessary to consider only those KT interventions that did not necessitate a significant increase in human resources. Consequently, the KT plan detailed in Table 3 was streamlined to include the minimum number of interventions necessary to address all key TDF domains (as per Fahim et al70).
The first KT intervention type “Education” focuses on a multi-faceted education approach, and aims to address the TDF domains detailed in Table 3.70 It employs multiple modes of education-focussed interventions that will be designed to address each of the targeted TDF domains; and will include a focus on the evidence supporting the safety and effectiveness of ACV and in-line PMVs. The evidence surrounding the effectiveness of multi-faceted education interventions in facilitating KT in healthcare settings is generally positive.75
The second intervention type “Enablement” targets the TDF domains detailed in Table 3.70 This intervention type will leverage champions who support, market and address resistance related to the use of ACV and in-line PMVs within the ICU. It will also utilise learning collaboratives and communities of practice within each relevant profession to deepen expertise and knowledge about these methods. The Global Tracheostomy Collaborative (GTC), of which the study centre is a member, is anticipated to be instrumental in creating, optimising, and sustaining these learning collaboratives. The GTC is a global community where a multi-disciplinary team of healthcare professionals are empowered to learn with a view to continuously improving the outcomes of patients with tracheostomies. The GTC’s ability to facilitate KT is evidenced by its previously demonstrated effectiveness in contributing to the swift implementation of ACV in other centres.27
In addition, patients who are being ventilated via a tracheostomy will be enabled to actively advocate for use of their preferred communication method, by ensuring they are aware of their rights to be involved in decision making regarding their care71; and through the provision of education and resources regarding available VAS methods.
Limitations
This study had a number of limitations. Participants were a self-selecting convenience sample drawn from relevant healthcare professionals working in Intensive Care. This introduced the risk of selection bias. In addition, the sample was drawn from a single Australian centre, thereby potentially limiting the generalisability of the study’s findings to other similar tertiary referral centres within Australia.
No published information regarding the psychometric properties of the TFA questionnaire used in this study exist. This reflects the developing nature of the questionnaire, with the questionnaire’s authors encouraging further work in this area.57
The order in which VAS methods were presented was not randomised, leading to an order effect evidenced by lower response rates for the questions relating to VALS and in-line PMVs. These questions were administered second and third (respectively). The presentation order did not appear to influence the acceptability results.
The use of free-text survey responses to collect information relating to the barriers and facilitators of VAS use resulted in the collection of information with limited depth. Collection of this information via interview would likely result in collection of more detailed responses.
This paper is the first to explore the factors that may be impacting on the routine use of VAS methods to facilitate communication in a vulnerable group of patients who are receiving ventilation via a tracheostomy.
Conclusion
Above Cuff Voicing (ACV), VALS and in-line PMVs were all deemed to be acceptable by relevant healthcare professionals working in Intensive Care. Above Cuff Voicing and in-line PMVs were deemed to be significantly more acceptable than VALS; with familiarity and perceptions regarding intervention safety theorised to impact upon their acceptability. In light of this, future research should prioritise the investigation of VALS safety, specifically in critical care contexts.
In Intensive Care settings, multi-disciplinary teams should consider the creation of KT intervention plans tailored to their specific context. These plans should be designed to address the key domains of the TDF as outlined in this paper. These domains serve as indicators of the high frequency barriers and facilitators that impact on the consistent adoption and use of VAS methods.
Financial support and sponsorship
This project was supported by a small research starter grant awarded by the Royal Hobart Hospital Department of Critical Care.
Conflicts of interest
None declared
Presentation
Preliminary findings from this study were presented at the Speech Pathology Australia National Conference (2023)